Puente Angela, Fortea Jose Ignacio, Posadas Miguel, Garcia Blanco Agustin, Rasines Laura, Cabezas Joaquin, Arias Loste Maria Teresa, Llerena Susana, Iruzubieta Paula, Fábrega Emilio, Crespo Javier
Digestive Disease Department, Marqués de Valdecilla University Hospital, 39008 Santander, Spain.
Health Research Institute Marques de Valdecilla, IDIVAL, 39011 Santander, Spain.
J Clin Med. 2019 Aug 17;8(8):1242. doi: 10.3390/jcm8081242.
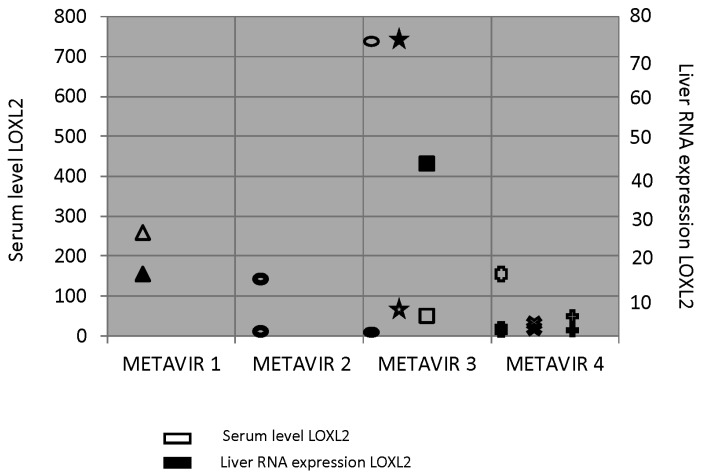
we aimed to assess the influence of metabolic syndrome on fibrosis regression (using liver-stiffness measurement (LSM) and serological scores) and the relationship with the expression of lysyl oxidase-like-2 as a potential goal of antifibrotic therapy.
We included 271 patients treated with Direct Antiviral Therapy (DAAs) in our hospital who achieved a sustained virological response (SVR); physical examination, blood tests, and LSM were made at baseline (B) and 24 months (24 M) after SVR. Hemodynamic studies and transjugular liver biopsies were performed on 13 patients.
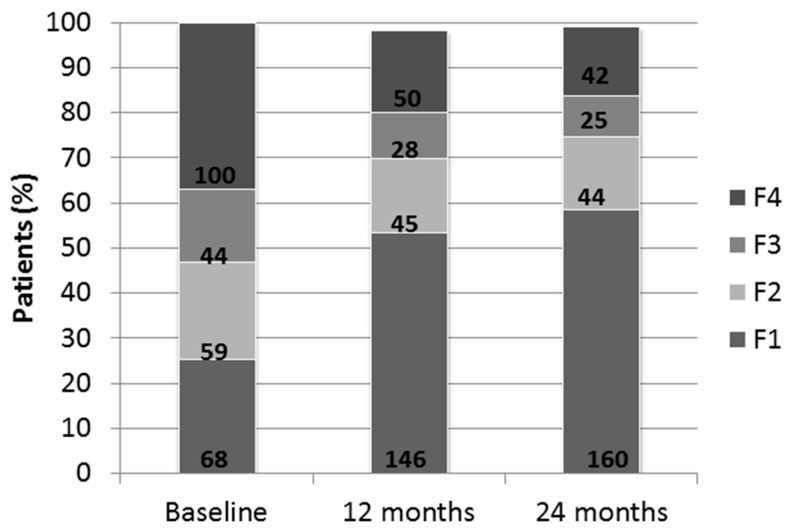
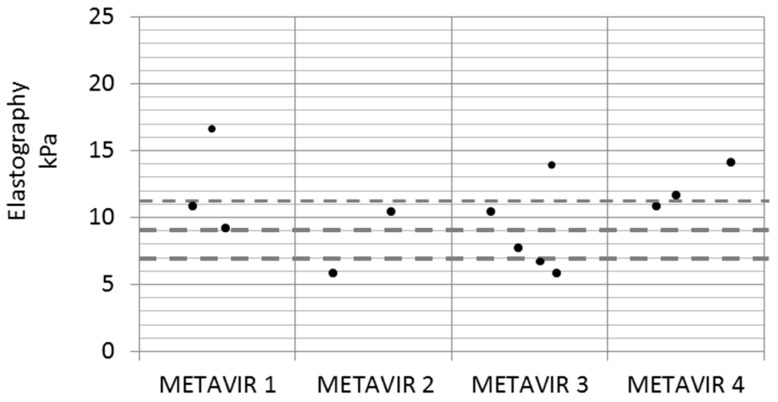
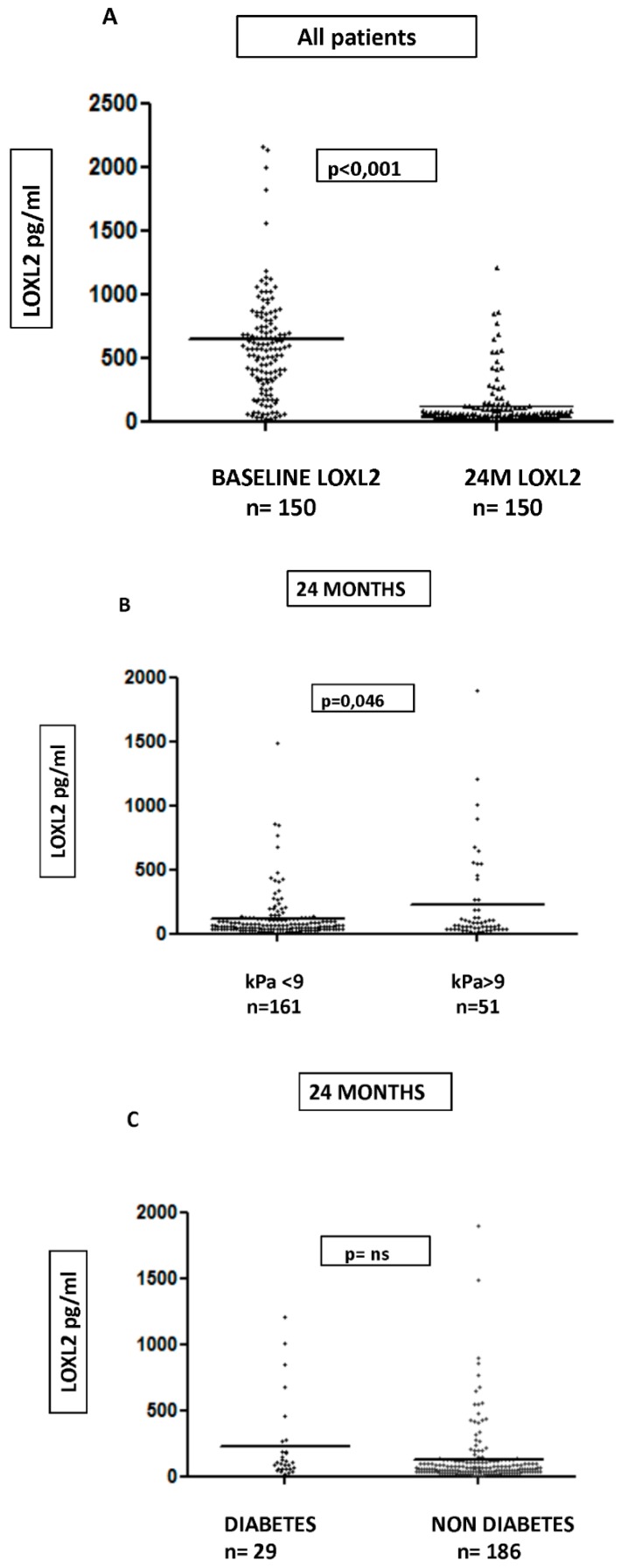
At B, 68 patients were F1 (25.1%); F2 = 59 (21.7%); F3 = 44 (16.05%); and 100 were F4 (36.9%). Although the LSM (absolute value) improved in 82% of patients ( = 222), it progressed in 17.5% of patients ( = 48). At 24 M, 48 patients met the metabolic syndrome (MetS) criteria and there was an increase in patients with a BMI of >25 kg/m ( < 0.001). At B and 24 M, a BMI of >25 kg/m is a risk factor for significant fibrosis or steatosis at 24 M ( < 0.05) and progression on LSM ( < 0.001), as well as MetS at B and 24 M (OR 4.1 IC (1.4-11.7), = 0.008; and OR 5.4 IC (1.9-15.4), = 0.001, respectively). Regarding the correlation between LSM and the liver biopsy, we found that only six out of 13 patients had a matching LSM and biopsy. We found a statistically significant decrease in LOXL2 levels at 24 M with respect to B ( < 0.001) with higher serological value in patients with elastography of >9 kPa vs. <9 kPa ( = 0.046).
Regression of LSM was reached in 82% of patients. Downregulated LOXL2 was demonstrated post-SVR, with overexpression in cirrhotic patients being a potential therapy goal in selected patients.
我们旨在评估代谢综合征对纤维化消退的影响(采用肝脏硬度测量(LSM)和血清学评分),以及与赖氨酰氧化酶样 2 表达的关系,将其作为抗纤维化治疗的潜在目标。
我们纳入了我院 271 例接受直接抗病毒治疗(DAA)并实现持续病毒学应答(SVR)的患者;在基线(B)和 SVR 后 24 个月(24M)进行体格检查、血液检查和 LSM。对 13 例患者进行了血流动力学研究和经颈静脉肝活检。
在基线时,68 例患者为 F1(25.1%);F2 = 59 例(21.7%);F3 = 44 例(16.05%);100 例为 F4(36.9%)。尽管 82%的患者(n = 222)LSM(绝对值)有所改善,但 17.5%的患者(n = 48)病情进展。在 24M 时,48 例患者符合代谢综合征(MetS)标准,且体重指数(BMI)>25 kg/m²的患者有所增加(P < 0.001)。在基线和 24M 时,BMI>25 kg/m²是 24M 时显著纤维化或脂肪变性的危险因素(P < 0.05)以及 LSM 进展的危险因素(P < 0.001),也是基线和 24M 时 MetS 的危险因素(OR 4.1,95%CI(1.4 - 11.7),P = 0.008;OR 5.4,95%CI(1.9 - 15.4),P = 0.001)。关于 LSM 与肝活检的相关性,我们发现 13 例患者中只有 6 例 LSM 与活检结果相符。我们发现 24M 时 LOXL2 水平相对于基线有统计学意义的下降(P < 0.001),弹性成像>9 kPa 的患者血清学值高于<9 kPa 的患者(P = 0.046)。
82%的患者实现了 LSM 的消退。SVR 后 LOXL2 表达下调,肝硬化患者的过表达是部分患者潜在的治疗目标。