Chang Emma M, Bretherick Andrew, Drummond Gordon B, Baillie J Kenneth
Anaesthesia, Critical Care and Pain Medicine, Royal Infirmary of Edinburgh, Edinburgh, EH16 4SA, UK.
MRC Institute of Genetics and Molecular Medicine, The University of Edinburgh, Edinburgh, EH4 2XU, UK.
Intensive Care Med Exp. 2019 Aug 20;7(1):49. doi: 10.1186/s40635-019-0262-1.
Accurate measurement of pulmonary oxygenation is important for classification of disease severity and quantification of outcomes in clinical studies. Currently, tension-based methods such as P/F ratio are in widespread use, but are known to be less accurate than content-based methods. However, content-based methods require invasive measurements or sophisticated equipment that are rarely used in clinical practice. We devised two new methods to infer shunt fraction from a single arterial blood gas sample: (1) a non-invasive effective shunt (ES) fraction calculated using a rearrangement of the indirect Fick equation, standard constants, and a procedural inversion of the relationship between content and tension and (2) inferred values from a database of outputs from an integrated mathematical model of gas exchange (DB). We compared the predictive validity-the accuracy of predictions of PO following changes in FO-of each measure in a retrospective database of 78,159 arterial blood gas (ABG) results from critically ill patients.
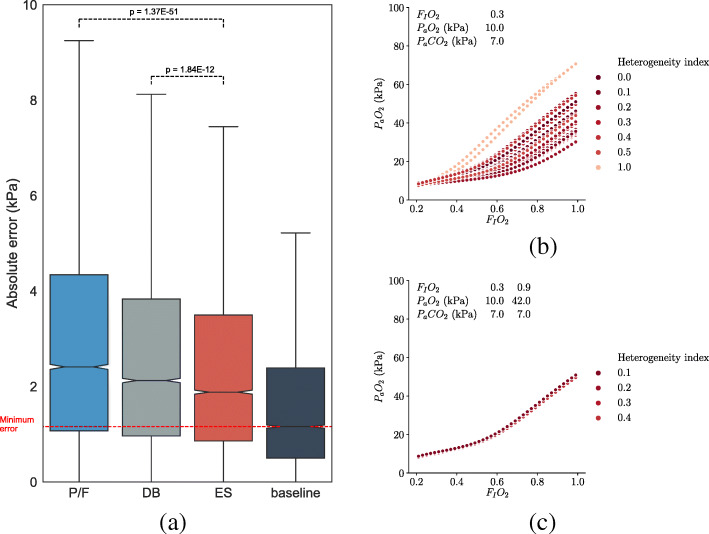
In a formal test set comprising 9,635 pairs of ABGs, the median absolute error (MAE) values for the four measures were as follows: alveolar-arterial difference, 7.30 kPa; PO/FO ratio, 2.41 kPa; DB, 2.13 kPa; and ES, 1.88 kPa. ES performed significantly better than other measures (p < 10-10 in all comparisons). Further exploration of the DB method demonstrated that obtaining two blood gas measurements at different FO provides a more precise description of pulmonary oxygenation.
Effective shunt can be calculated using a computationally efficient procedure using routinely collected arterial blood gas data and has better predictive validity than other analytic methods. For practical assessment of oxygenation in clinical research, ES should be used in preference to other indices. ES can be calculated at http://baillielab.net/es .
准确测量肺氧合对于疾病严重程度的分类以及临床研究中结果的量化至关重要。目前,基于张力的方法如P/F比值被广泛使用,但已知其准确性低于基于含量的方法。然而,基于含量的方法需要侵入性测量或复杂设备,而这些在临床实践中很少使用。我们设计了两种从单一动脉血气样本推断分流分数的新方法:(1)一种无创有效分流(ES)分数,使用间接Fick方程的重新排列、标准常数以及含量与张力关系的程序反转来计算;(2)从气体交换综合数学模型输出的数据库(DB)中推断的值。我们在一个包含78159例危重症患者动脉血气(ABG)结果的回顾性数据库中,比较了每种测量方法在吸入氧分数(FO)变化后对动脉血氧分压(PO)预测变化——预测有效性的准确性。
在一个由9635对ABG组成的正式测试集中,四种测量方法的中位数绝对误差(MAE)值如下:肺泡 - 动脉氧分压差为7.30kPa;PO/FO比值为2.41kPa;DB为2.13kPa;ES为1.88kPa。ES的表现明显优于其他测量方法(所有比较中p < 10⁻¹⁰)。对DB方法的进一步探索表明,在不同FO下获取两次血气测量能更精确地描述肺氧合情况。
有效分流可通过使用常规收集的动脉血气数据的计算高效程序来计算,并且比其他分析方法具有更好的预测有效性。对于临床研究中氧合的实际评估,应优先使用ES而非其他指标。可在http://baillielab.net/es计算ES值。