Pertl Maria M, Sooknarine-Rajpatty Aditi, Brennan Sabina, Robertson Ian H, Lawlor Brain A
Royal College of Surgeons in Ireland, Dublin, Ireland.
Trinity College Institute of Neuroscience, Trinity College Dublin, Dublin, Ireland.
Front Psychol. 2019 Aug 13;10:1801. doi: 10.3389/fpsyg.2019.01801. eCollection 2019.
The perception of choice in becoming a caregiver may impact on caregiver psychological and physical health. We determined the proportion of spousal dementia caregivers who felt they had a choice, and examined whether lack of choice in taking up the caregiving role and the perceived degree of choice in caregiving predicted caregiver health and wellbeing and care-recipient placement in long-term care at 1-year follow-up.
We performed secondary analyses of data from DeStress, a longitudinal study of 251 spousal dementia caregivers in Ireland. We used multivariate logistic and linear regression analyses to examine whether lack of choice (a dichotomous item) and/or the perceived degree of choice (a 9-point scale) at baseline predicted caregiver health (number of chronic health conditions; self-reported health) and wellbeing (e.g., burden, anxiety, depression, stress, and positive aspects of caregiving) and care status (continued care at home or placement in long-term care) at follow-up.
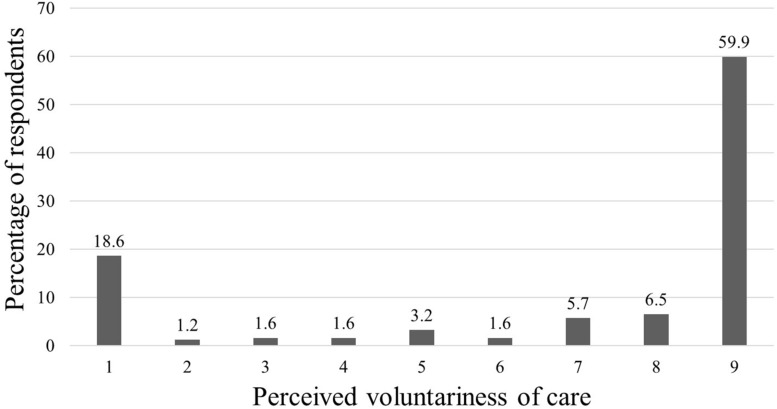
The vast majority of caregivers (82%) reported that they had no choice in taking up the caregiving role. Nevertheless, nearly three-quarters (74%) responded above the midpoint on the rating scale (Mean = 6.82, = 3.22; Median = 9; Mode = 9), indicating they provided care voluntarily. Caregivers who reported a greater degree of choice were more likely to still be providing care at home at follow-up and to identify benefits from providing care. Neither choice nor degree of choice predicted any other caregiver outcomes.
For the vast majority of spousal dementia caregivers, taking up the caregiving role is not perceived as a choice; yet, most report performing this role voluntarily. Thus, facilitating greater choice may not necessarily diminish the key contribution family caregivers make to the care system. Although we found no evidence that caregiver choice predicted more positive caregiver health and wellbeing, the perception of choice is important in and of itself, and may benefit caregivers by facilitating the identification of positive aspects of care and be a factor in delaying care-recipient placement in long-term care. Future research should be especially mindful of how caregiver choice is assessed and how this may affect the resulting prevalence of choice.
成为照料者时对选择的认知可能会影响照料者的心理和身体健康。我们确定了认为自己有选择的配偶痴呆症照料者的比例,并研究了在承担照料角色时缺乏选择以及在照料过程中感知到的选择程度是否能预测在1年随访时照料者的健康和幸福状况以及照料对象在长期护理机构的安置情况。
我们对来自爱尔兰一项针对251名配偶痴呆症照料者的纵向研究DeStress的数据进行了二次分析。我们使用多变量逻辑回归和线性回归分析来检验基线时缺乏选择(一个二分项目)和/或感知到的选择程度(一个9分制量表)是否能预测随访时照料者的健康状况(慢性健康状况的数量;自我报告的健康状况)和幸福状况(如负担、焦虑、抑郁、压力以及照料的积极方面)以及照料状态(继续在家照料或安置在长期护理机构)。
绝大多数照料者(82%)报告称他们在承担照料角色时没有选择。然而,近四分之三(74%)的人在评分量表上的回答高于中点(均值 = 6.82,标准差 = 3.22;中位数 = 9;众数 = 9),表明他们是自愿提供照料的。报告有更大选择程度的照料者在随访时更有可能仍在家中提供照料,并能从提供照料中发现益处。选择或选择程度均未预测任何其他照料者的结果。
对于绝大多数配偶痴呆症照料者来说,承担照料角色不被视为一种选择;然而,大多数人报告是自愿履行这一角色的。因此,提供更多选择不一定会减少家庭照料者对护理系统的关键贡献。尽管我们没有发现证据表明照料者的选择能预测更积极的照料者健康和幸福状况,但选择的认知本身很重要,可能会通过促使照料者识别照料的积极方面而使他们受益,并且可能是延迟照料对象安置到长期护理机构的一个因素。未来的研究应特别注意照料者选择是如何评估的以及这可能如何影响选择的结果发生率。