Pfizer Limited, Walton Oaks, Dorking Road, Walton-on-the-Hill, Tadworth, Surrey, KT20 7NS, UK.
Barts Heart Centre, St Bartholomew's Hospital, London, UK.
ESC Heart Fail. 2019 Oct;6(5):1041-1051. doi: 10.1002/ehf2.12511. Epub 2019 Sep 5.
The study aims to systematically assess the diagnostic performance of cardiac magnetic resonance (CMR) and nuclear scintigraphy (index tests) for the diagnosis and differentiation of subtypes of cardiac amyloidosis.
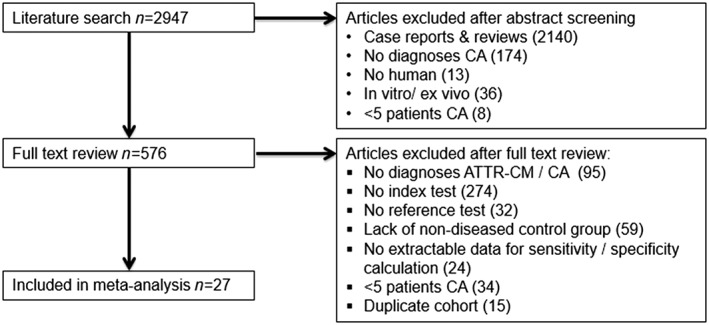
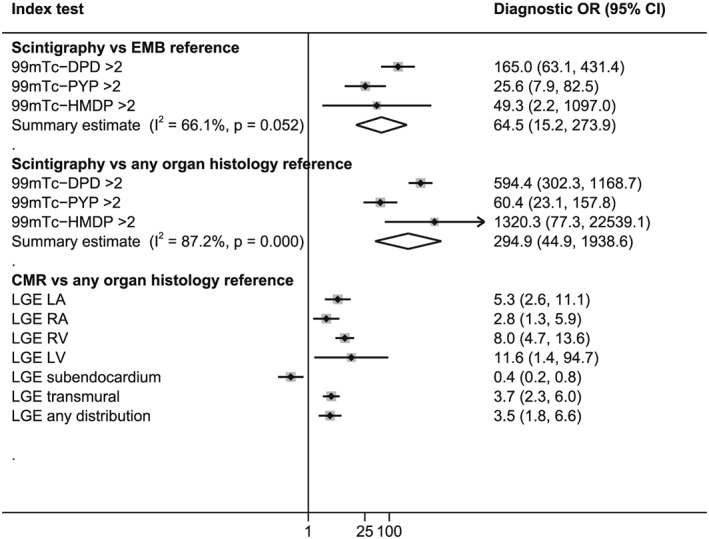
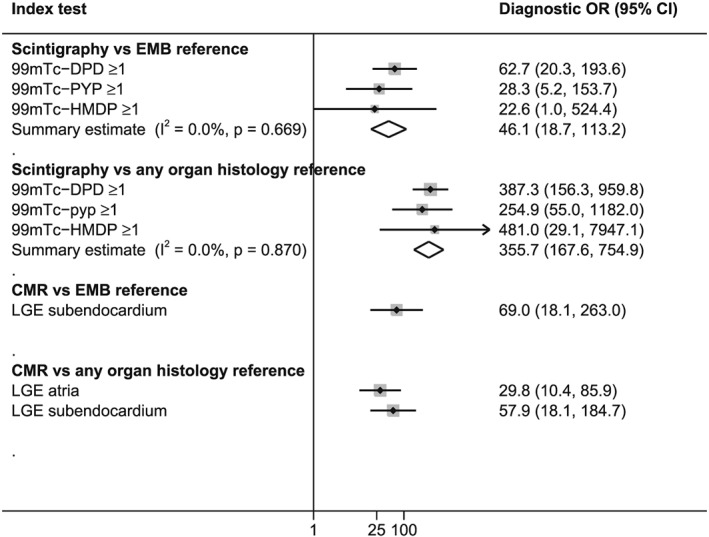
MEDLINE and Embase electronic databases were searched for studies evaluating the diagnostic performance of CMR or nuclear scintigraphy in detecting cardiac amyloidosis and subsequently in differentiating transthyretin amyloidosis (ATTR) from immunoglobulin light-chain (AL) amyloidosis. In this meta-analysis, histopathological examination of tissue from endomyocardial biopsy (EMB) or extra-cardiac organs were reference standards. Pooled sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio were calculated, and a random effects meta-analysis was used to estimate diagnostic odds ratios. Methodological quality was assessed using a validated instrument. Of the 2947 studies identified, 27 met the criteria for inclusion. Sensitivity and specificity of CMR in diagnosing cardiac amyloidosis was 85.7% and 92.0% against EMB reference and 78.9% and 93.9% with any organ histology reference. Corresponding sensitivity and specificity of nuclear scintigraphy was 88.4% and 87.2% against EMB reference and 82.0% and 98.8% with histology from any organ. CMR was unable to reliably differentiate ATTR from AL amyloidosis (sensitivity 28.1-99.0% and specificity 11.0-60.0%). Sensitivity and specificity of nuclear scintigraphy in the differentiation of ATTR from AL amyloidosis ranged from 90.9% to 91.5% and from 88.6% to 97.1%. Pooled negative likelihood ratio and positive likelihood ratio for scintigraphy in this setting were 0.1 and 8, with EMB reference standard. Study quality assessed by QUADAS-2 was generally poor with evidence of bias.
Cardiac magnetic resonance is a useful test for diagnosing cardiac amyloidosis but is not reliable in further classifying the disease. Nuclear scintigraphy offers strong diagnostic performance in both the detection of cardiac amyloidosis and differentiating ATTR from AL amyloidosis. Our findings support the use of both imaging modalities in a non-invasive diagnostic algorithm that also tests for the presence of monoclonal protein.
本研究旨在系统评估心脏磁共振(CMR)和核闪烁显像(指数试验)在诊断和区分心脏淀粉样变性亚型方面的诊断性能。
检索 MEDLINE 和 Embase 电子数据库,评估 CMR 或核闪烁显像在诊断心脏淀粉样变性以及随后区分转甲状腺素淀粉样变性(ATTR)与免疫球蛋白轻链(AL)淀粉样变性方面的诊断性能的研究。在这项荟萃分析中,组织学检查来自心内膜心肌活检(EMB)或心脏外器官的组织为参考标准。计算合并的敏感性、特异性、阳性似然比和阴性似然比,并使用随机效应荟萃分析估计诊断比值比。使用经过验证的工具评估方法学质量。在确定的 2947 项研究中,有 27 项符合纳入标准。CMR 诊断心脏淀粉样变性的敏感性和特异性分别为 85.7%和 92.0%,与 EMB 参考标准相对应,敏感性和特异性分别为 78.9%和 93.9%,与任何器官组织学参考标准相对应。核闪烁显像的相应敏感性和特异性分别为 88.4%和 87.2%,与 EMB 参考标准相对应,敏感性和特异性分别为 82.0%和 98.8%,与任何器官的组织学参考标准相对应。CMR 无法可靠地区分 ATTR 与 AL 淀粉样变性(敏感性 28.1-99.0%和特异性 11.0-60.0%)。核闪烁显像在区分 ATTR 与 AL 淀粉样变性方面的敏感性和特异性范围分别为 90.9%-91.5%和 88.6%-97.1%。在这种情况下,核闪烁显像的合并阴性似然比和阳性似然比分别为 0.1 和 8,参考标准为 EMB。使用 QUADAS-2 评估的研究质量普遍较差,存在偏倚证据。
心脏磁共振是一种有用的诊断心脏淀粉样变性的检测方法,但在进一步对疾病进行分类方面不可靠。核闪烁显像在诊断心脏淀粉样变性和区分 ATTR 与 AL 淀粉样变性方面均具有良好的诊断性能。我们的研究结果支持在一种非侵入性诊断算法中同时使用这两种影像学方法,该算法还可检测单克隆蛋白的存在。