Department of Orthopedics, Peking University Third Hospital, Beijing, China.
Eight-Year-Program, Grade 2015, Health Science Center, Peking University, Beijing, China.
Cancer Med. 2019 Oct;8(14):6176-6184. doi: 10.1002/cam4.2546. Epub 2019 Sep 5.
In the treatment of spinal metastases, stereotactic body radiotherapy (SBRT) delivers precise, high-dose radiation to the target region while sparing the spinal cord. A range of doses and fractions had been reported; however, the optimal prescribed scheme remains unclear.
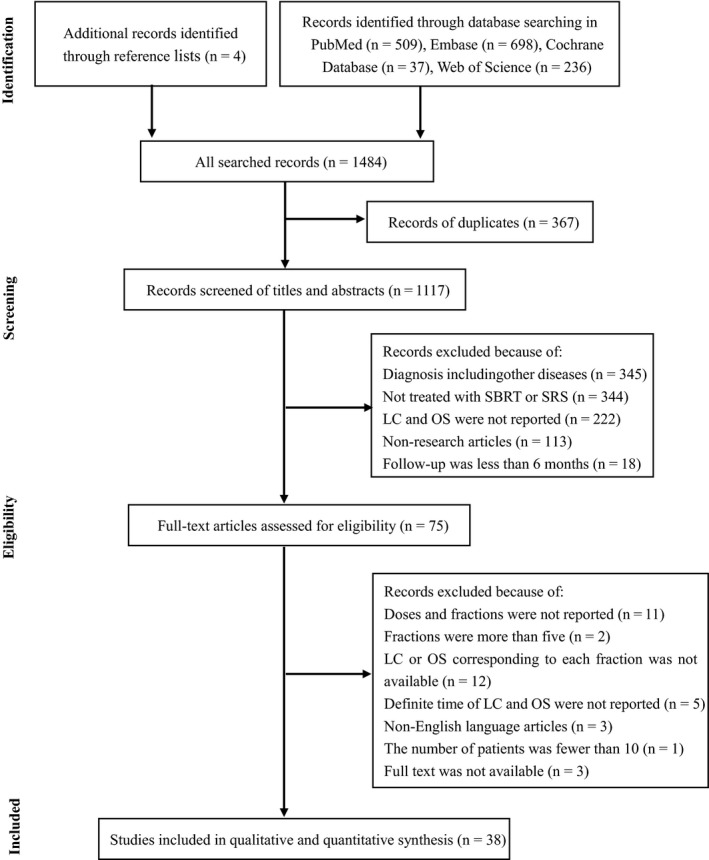
Two reviewers performed independent literature searches of the PubMed, EMBASE, Cochrane Database, and Web of Science databases. Articles were divided into one to five fractions groups. The Methodological Index for Non-randomized Studies (MINORS) was used to assess the quality of studies. Local control (LC) and overall survival (OS) were presented for the included studies and a pooled value was calculated by the weighted average.
The 38 included studies comprised 3,754 patients with 4,731 lesions. The average 1-year LCs for the one to five fractions were 92.7%, 84.6%, 86.8%, 82.6%, and 80.6%, respectively. The average 1-year OS for the one to five fractions were 53.0%, 70.4%, 60.1%, 48%, and 80%, respectively. The 24 Gy/single fraction scheme had a higher 1-year LC (98.1%) than those of 24 Gy/two fractions (85.4%), 27 Gy/three fractions (84.9%), and 24 Gy/three fractions (89.0%). The incidence of vertebral compression fracture was 10.3%, with 10.7% in the single-fraction group and 10.1% in the multi-fraction group. The incidence of radiation-induced myelopathy was 0.19%; three and two patients were treated with single-fraction and multi-fraction SBRT, respectively. The incidence of radiculopathy was 0.30% and all but one patient were treated with multi-fraction SBRT.
SBRT provided satisfactory efficacy and acceptable safety for spinal metastases. Single-fraction SBRT demonstrated a higher local control rate than those of the other factions, especially the 24 Gy dose. The risk of vertebral compression fracture (VCF) was slightly higher in single-fraction SBRT and more patients developed radiculopathy after multi-fraction SBRT.
在脊柱转移瘤的治疗中,立体定向体部放疗(SBRT)能够精确地将高剂量辐射送达靶区,同时保护脊髓。目前已经报道了多种剂量和分割方案,但最佳的处方方案仍不明确。
两位审稿人独立检索了 PubMed、EMBASE、Cochrane 数据库和 Web of Science 数据库中的文献。文章被分为 1 至 5 个分割组。采用非随机研究方法学指数(MINORS)评估研究质量。纳入研究报告局部控制(LC)和总生存(OS),并通过加权平均计算汇总值。
38 项纳入研究共包含 3754 例患者和 4731 个病灶。1 年时,1 至 5 个分割组的 1 年 LC 分别为 92.7%、84.6%、86.8%、82.6%和 80.6%。1 年 OS 分别为 53.0%、70.4%、60.1%、48%和 80%。24 Gy/单次分割方案的 1 年 LC(98.1%)高于 24 Gy/2 次分割(85.4%)、27 Gy/3 次分割(84.9%)和 24 Gy/3 次分割(89.0%)。椎体压缩性骨折的发生率为 10.3%,单次分割组为 10.7%,多次分割组为 10.1%。放射性脊髓病的发生率为 0.19%;3 例和 2 例患者分别接受了单次分割和多次分割 SBRT 治疗。神经根病的发生率为 0.30%,且所有患者均接受了多次分割 SBRT 治疗。
SBRT 为脊柱转移瘤提供了满意的疗效和可接受的安全性。单次分割 SBRT 的局部控制率高于其他分割组,尤其是 24 Gy 剂量。单次分割 SBRT 的椎体压缩性骨折(VCF)风险略高,且多次分割 SBRT 后更多患者出现神经根病。