Department of Medicine, High Altitude Medical Research Centre, Leh, Ladakh, India.
Military Nursing Services, Integrated HQ, Ministry of Defence, New Delhi, India.
Indian J Med Res. 2019 Jun;149(6):778-782. doi: 10.4103/ijmr.IJMR_1981_17.
BACKGROUND & OBJECTIVES: High-altitude pulmonary oedema (HAPE) continues to challenge the healthcare providers at remote, resource-constrained settings. High-altitude terrain itself precludes convenience of resources. This study was conducted to evaluate the rise in peripheral capillary saturation of oxygen (SpO) by the use of a partial rebreathing mask (PRM) in comparison to Hudson's mask among patients with HAPE.
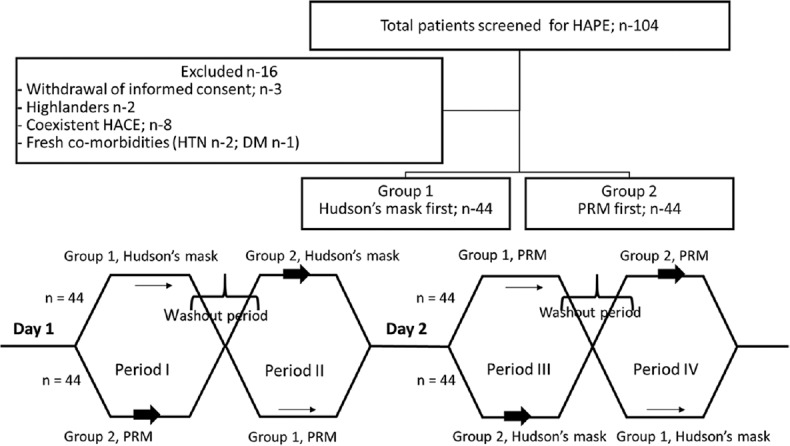
This was a single-centre, randomized crossover study to determine the efficiency of PRM in comparison to Hudson's mask. A total of 88 patients with HAPE referred to a secondary healthcare facility at an altitude of 11,500 feet from January to October 2013 were studied. A crossover after adequate wash-out on both modalities was conducted for first two days of hospital admission. All patients with HAPE were managed with bed rest and stand-alone oxygen supplementation with no adjuvant pharmacotherapy.
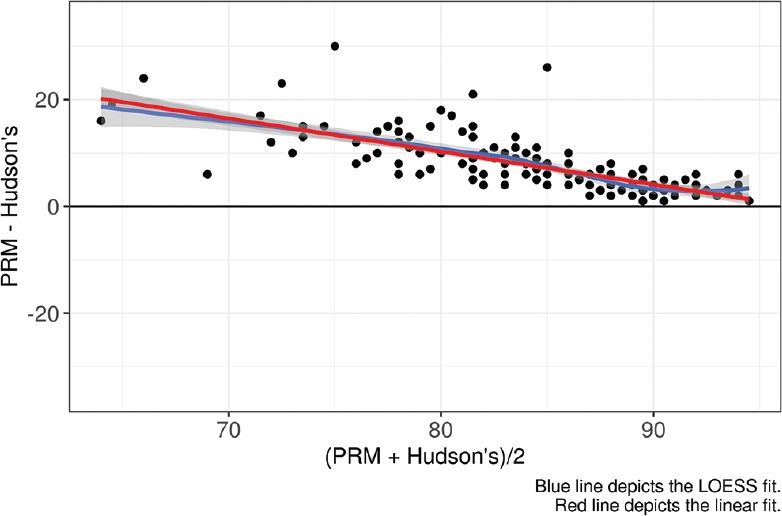
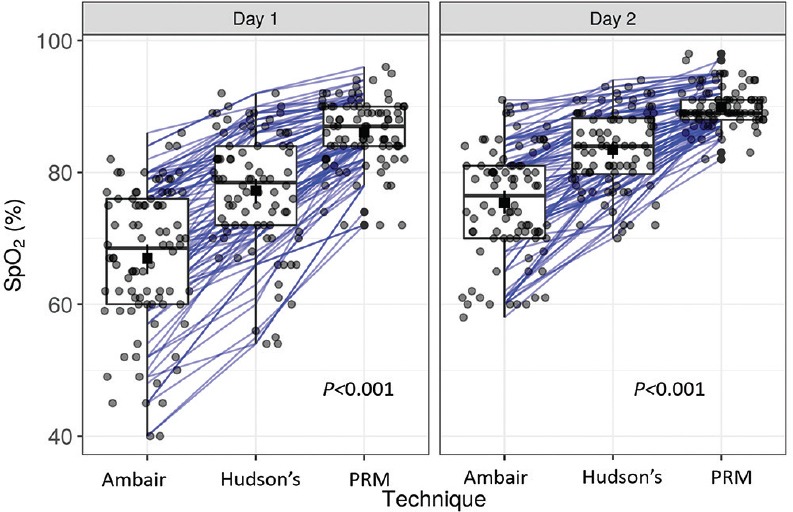
The mean SpOon ambient air on arrival was 66.92±10.8 per cent for all patients with HAPE. Higher SpOvalues were achieved with PRM in comparison to Hudson's mask on day one (86.08±5.15 vs. 77.23±9.09%) and day two (89.94±2.96 vs. 83.39±5.93%). The difference was more pronounced on day one as compared to day two.
INTERPRETATION & CONCLUSIONS: Mean SpOvalues were found to be significantly higher among HAPE patients using PRM compared to those on Hudson's mask. Further studies to understand the translation of this incremental response in SpOto clinical benefits (recovery times, mortality rates and hospital stay) need to be undertaken.
高原肺水肿(HAPE)在资源有限的偏远地区仍然对医疗保健提供者构成挑战。高原地形本身就妨碍了资源的便利性。本研究旨在评估使用部分重呼吸面罩(PRM)与 Hudson 面罩相比,在 HAPE 患者中升高外周毛细血管血氧饱和度(SpO)的效果。
这是一项单中心、随机交叉研究,旨在比较 PRM 与 Hudson 面罩的效率。2013 年 1 月至 10 月,共有 88 名 HAPE 患者被转诊至海拔 11500 英尺的二级医疗机构,对其进行研究。在两种模式下充分冲洗后,在住院的前两天进行交叉。所有 HAPE 患者均接受卧床休息和单独吸氧治疗,不使用辅助药物治疗。
所有 HAPE 患者到达时的平均 SpO 值在环境空气中为 66.92±10.8%。与 Hudson 面罩相比,PRM 在第一天(86.08±5.15%比 77.23±9.09%)和第二天(89.94±2.96%比 83.39±5.93%)都能获得更高的 SpO 值。第一天的差异比第二天更为明显。
与使用 Hudson 面罩的 HAPE 患者相比,使用 PRM 的 HAPE 患者的平均 SpO 值明显更高。需要进一步研究以了解 SpO 这种递增反应在临床获益(恢复时间、死亡率和住院时间)方面的转化。