Tufts Center for Clinical Evidence Synthesis, Institute for Clinical Research and Health Policy Studies, Tufts Medical Center, Boston, MA, USA.
Tufts University Friedman School of Nutrition Science and Policy, Boston, MA, USA.
Am J Clin Nutr. 2019 Nov 1;110(5):1067-1078. doi: 10.1093/ajcn/nqz178.
Although available data suggest that some dietary flavan-3-ol sources reduce cardiometabolic risk, to our knowledge no review has systematically synthesized their specific contribution.
We aimed to examine, for the first time, if there is consistent evidence that higher flavan-3-ol intake, irrespective of dietary source, reduces cardiometabolic risk.
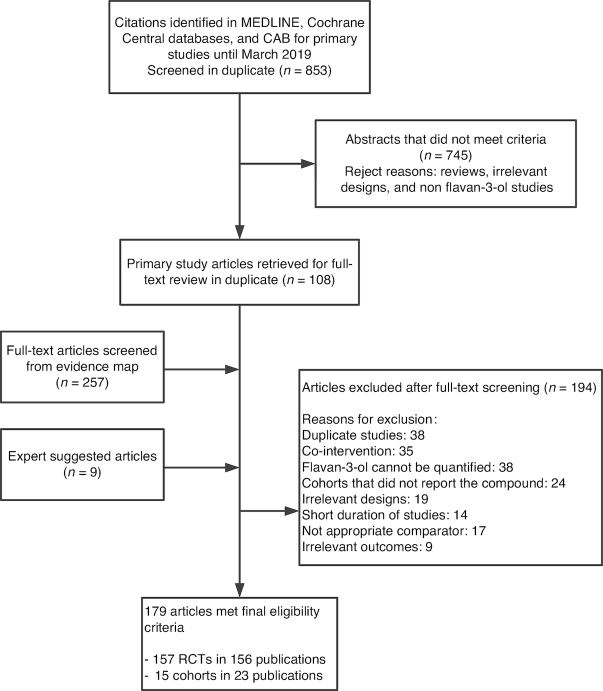
MEDLINE, Cochrane Central, and Commonwealth Agricultural Bureau abstracts were searched for prospective cohorts and randomized controlled trials (RCTs) published from 1946 to March 2019 on flavan-3-ol intake and cardiovascular disease (CVD) risk. Random-effects models meta-analysis was used. The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach assessed the strength of evidence.
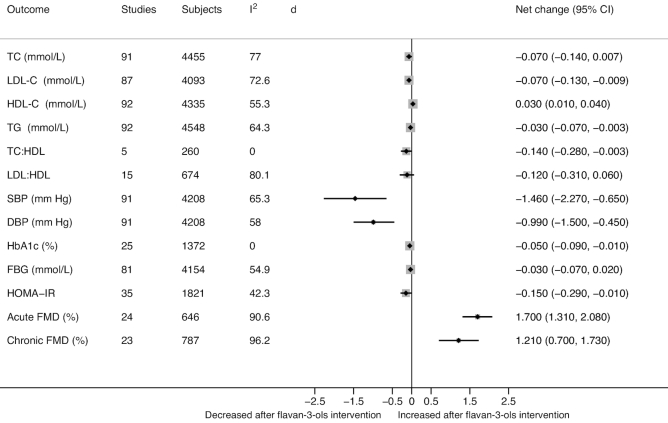
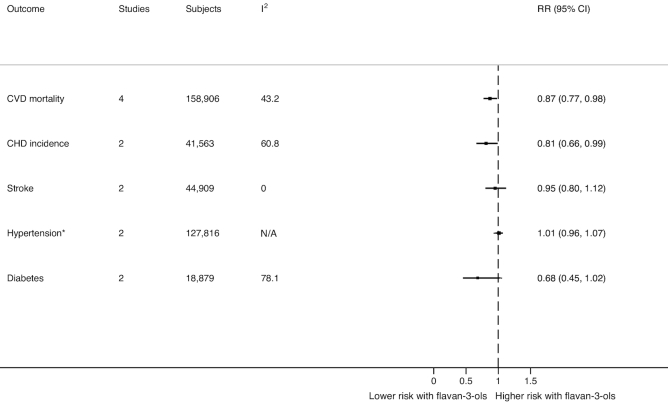
Of 15 prospective cohorts (23 publications), 4 found highest compared with lowest habitual intakes of flavan-3-ols were associated with a 13% reduction in risk of CVD mortality and 2 found a 19% reduction in risk of chronic heart disease (CHD) incidence. Highest compared with lowest habitual intakes of monomers were associated with a reduction in risk of type 2 diabetes mellitus (T2DM) (n = 5) and stroke (n = 4) (10% and 18%, respectively). No association was found for hypertension. Of 156 RCTs, flavan-3-ol intervention resulted in significant improvements in acute/chronic flow-mediated dilation (FMD), systolic (SBP) and diastolic blood pressure (DBP), total cholesterol (TC), LDL and HDL cholesterol, triglycerides (TGs), hemoglobin A1c (HbA1c), and homeostasis model assessment of insulin resistance (HOMA-IR). All analyses, except HbA1c, were associated with moderate/high heterogeneity. When analyses were limited to good methodological quality studies, improvements in TC, HDL cholesterol, SBP, DBP, HOMA-IR, and acute/chronic FMD remained significant. In GRADE evaluations, there was moderate evidence in cohort studies that flavan-3-ol and monomer intakes were associated with reduced risk of CVD mortality, CHD, stroke, and T2DM, whereas RCTs reported improved TC, HDL cholesterol, SBP, and HOMA-IR.
Available evidence supports a beneficial effect of flavan-3-ol intake on cardiometabolic outcomes, but there was considerable heterogeneity in the meta-analysis. Future research should focus on an integrated intake/biomarker approach in cohorts and high-quality dose-response RCTs. This review was registered at www.crd.york.ac.uk/PROSPERO/ as CRD42018035782.
虽然现有数据表明,一些富含黄烷-3-醇的食物来源可以降低心血管代谢风险,但据我们所知,还没有研究系统地综合评估其具体作用。
我们旨在首次检验摄入黄烷-3-醇(无论其来源如何)是否可以降低心血管代谢风险,这种作用是否有一致性证据。
检索了 1946 年至 2019 年 3 月期间发表的关于黄烷-3-醇摄入量与心血管疾病(CVD)风险的前瞻性队列研究和随机对照试验(RCT)的 MEDLINE、Cochrane 中心和英联邦农业局摘要。使用随机效应模型进行荟萃分析。采用 Grading of Recommendations Assessment, Development, and Evaluation(GRADE)方法评估证据的强度。
在 15 项前瞻性队列研究(23 项研究)中,有 4 项研究发现,最高与最低习惯性黄烷-3-醇摄入量相比,CVD 死亡率降低了 13%,有 2 项研究发现,慢性心脏病(CHD)发病率降低了 19%。单体摄入量最高与最低相比,2 型糖尿病(T2DM)风险降低了 10%(n=5),中风风险降低了 18%(n=4)。高血压无相关性。在 156 项 RCT 中,黄烷-3-醇干预可显著改善急性/慢性血流介导的扩张(FMD)、收缩压(SBP)和舒张压(DBP)、总胆固醇(TC)、低密度脂蛋白胆固醇(LDL-C)和高密度脂蛋白胆固醇(HDL-C)、甘油三酯(TGs)、糖化血红蛋白 A1c(HbA1c)和稳态模型评估的胰岛素抵抗(HOMA-IR)。除了 HbA1c,所有分析均存在中度/高度异质性。当分析仅限于方法学质量良好的研究时,TC、HDL-C、SBP、DBP、HOMA-IR 和急性/慢性 FMD 的改善仍具有统计学意义。在 GRADE 评估中,队列研究中有中等证据表明,黄烷-3-醇和单体摄入量与 CVD 死亡率、CHD、中风和 T2DM 风险降低有关,而 RCT 报告了 TC、HDL-C、SBP 和 HOMA-IR 的改善。
现有证据支持黄烷-3-醇摄入量对心血管代谢结局有益,但荟萃分析存在较大异质性。未来的研究应侧重于队列研究中的综合摄入量/生物标志物方法和高质量的剂量反应 RCT。本综述已在 www.crd.york.ac.uk/PROSPERO/ 上注册,注册号为 CRD42018035782。