From the Immunology Clinic and Department of Neurology (A.B.), Departments of Medicine, Biomedicine and Clinical Research, University Hospital Basel; Department of Rheumatology (V.K.J., T.D.), University Hospital Basel, Switzerland; Department of Neurology (R.D.M.H.), King's College Hospital, London; Nuffield Department of Orthopedics (R.A.L., A.C.), Rheumatology and Musculoskeletal Sciences, Botnar Research Centre, University of Oxford, United Kingdom; Department of Neurology (A.-K.P.), University Hospital Basel & Clinical Neuroimmunology; Department of Biomedicine (A.-K.P.), University of Basel, Switzerland; Division of Rheumatology and Department of Biostatistics, Epidemiology, and Informatics (P.A.M.), University of Pennsylvania, Philadelphia; Department of Rheumatology (R.S.), Auckland District Health Board, New Zealand; and Department of Neurology (M.P.C.), Medical College of Wisconsin, Milwaukee, WI.
Neurol Neuroimmunol Neuroinflamm. 2019 Sep 20;6(6). doi: 10.1212/NXI.0000000000000615. Print 2019 Nov.
Reported prevalence of vasculitic neuropathy (VN) in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is highly variable, and associations with other organ manifestations have not been studied systematically while accounting for diagnostic certainty of VN.
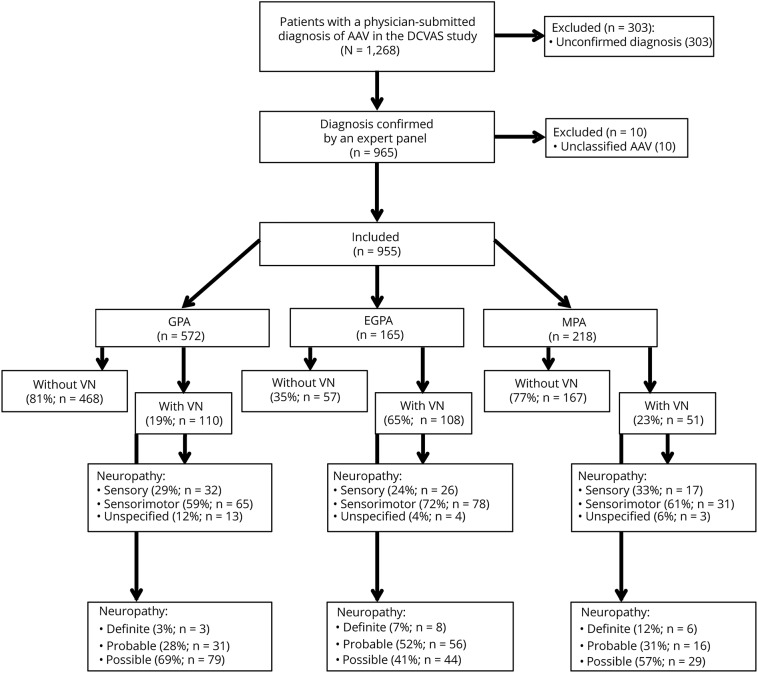
Data of all patients with AAV within the Diagnostic and Classification criteria for primary systemic VASculitis study were analyzed cross-sectionally. VN was categorized as definite (histology proven), probable (multiple mononeuropathy or nerve biopsy consistent with vasculitis), or possible (all others). Associations with other organ manifestations were compared in patients with and without VN.
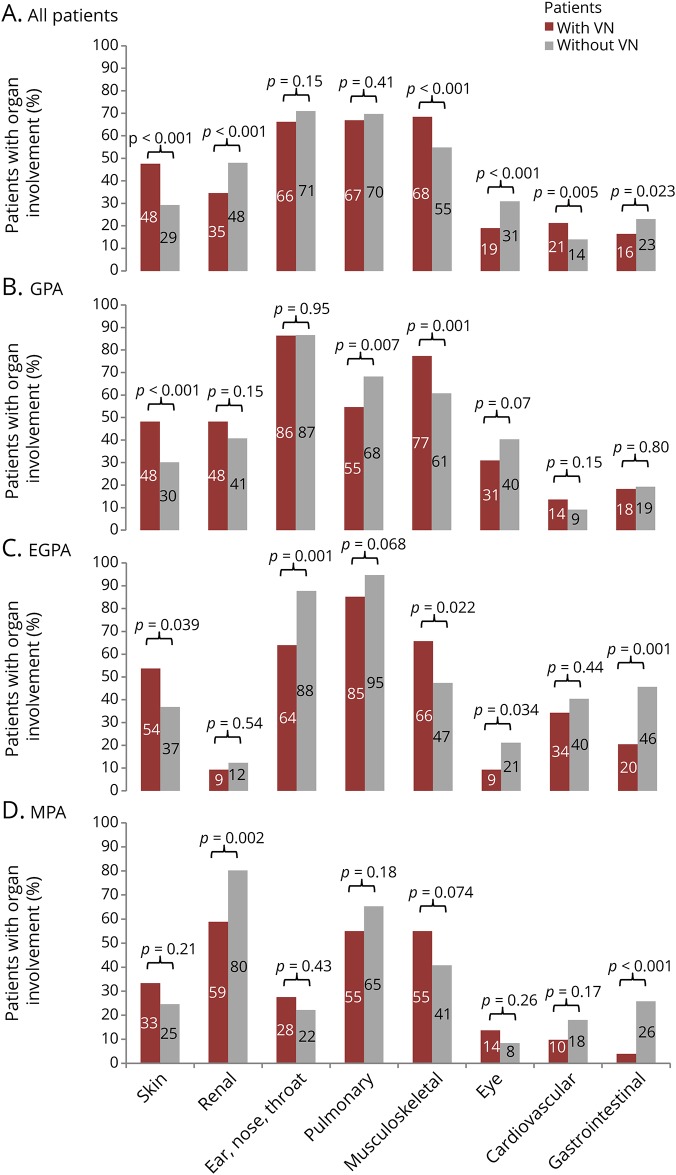
Nine hundred fifty-five patients (mean age 57 years, range 18-91 years, 51% female) were identified. Of these, 572 had granulomatosis with polyangiitis (GPA), 218 microscopic polyangiitis (MPA), and 165 eosinophilic granulomatosis with polyangiitis (EGPA). The prevalence of VN was 65% in EGPA, 23% in MPA, and 19% in GPA. Nerve biopsy was performed in 32/269 (12%) patients, demonstrating definite vasculitis in 17/32 (53%) of patients. VN was associated with myeloperoxidase-ANCA positivity ( 0.004) and skin ( < 0.001), musculoskeletal, ( < 0.001) and cardiovascular ( 0.005) involvement. Patients with VN were less likely to have renal ( < 0.001), eye ( < 0.001), and gastrointestinal ( 0.023) involvement.
Our study provides comprehensive insights into the prevalence and organ associations of VN in a large, systematically collected AAV cohort. VN is most commonly associated with skin, musculoskeletal, and cardiovascular manifestations. In routine clinical practice, diagnosis of VN is infrequently confirmed by the gold standard of nerve biopsy but rather supported by the clinical setting of active systemic AAV.
抗中性粒细胞胞浆抗体(ANCA)相关性血管炎(AAV)中血管炎性神经病(VN)的报道患病率差异很大,并且在考虑 VN 的诊断确定性的情况下,尚未系统地研究与其他器官表现的关联。
对原发性系统性血管炎诊断和分类标准研究中所有 AAV 患者的数据进行了横断面分析。VN 分为明确(组织学证实)、可能(多发性单神经病或神经活检符合血管炎)或可能(其他所有情况)。比较 VN 患者和无 VN 患者的其他器官表现。
共确定了 955 例患者(平均年龄 57 岁,范围 18-91 岁,51%为女性)。其中,572 例为肉芽肿性多血管炎(GPA),218 例为显微镜下多血管炎(MPA),165 例为嗜酸性肉芽肿性多血管炎(EGPA)。EGPA 的 VN 患病率为 65%,MPA 为 23%,GPA 为 19%。对 269 例患者中的 32 例(12%)进行了神经活检,其中 17 例(53%)证实为明确的血管炎。VN 与髓过氧化物酶-ANCA 阳性( 0.004)和皮肤( < 0.001)、肌肉骨骼( < 0.001)和心血管( 0.005)受累相关。VN 患者发生肾脏( < 0.001)、眼部( < 0.001)和胃肠道( 0.023)受累的可能性较低。
我们的研究提供了在一个大的、系统收集的 AAV 队列中 VN 的患病率和器官相关性的综合见解。VN 最常与皮肤、肌肉骨骼和心血管表现相关。在常规临床实践中,VN 的诊断很少通过神经活检的金标准得到证实,而是通过活动性系统性 AAV 的临床背景得到支持。