Department of Medicine, University of California at San Francisco, San Francisco, CA, United States of America.
Division of Environmental Health Sciences, School of Public Health, University of California, Berkeley, CA, United States of America.
PLoS One. 2019 Sep 25;14(9):e0222601. doi: 10.1371/journal.pone.0222601. eCollection 2019.
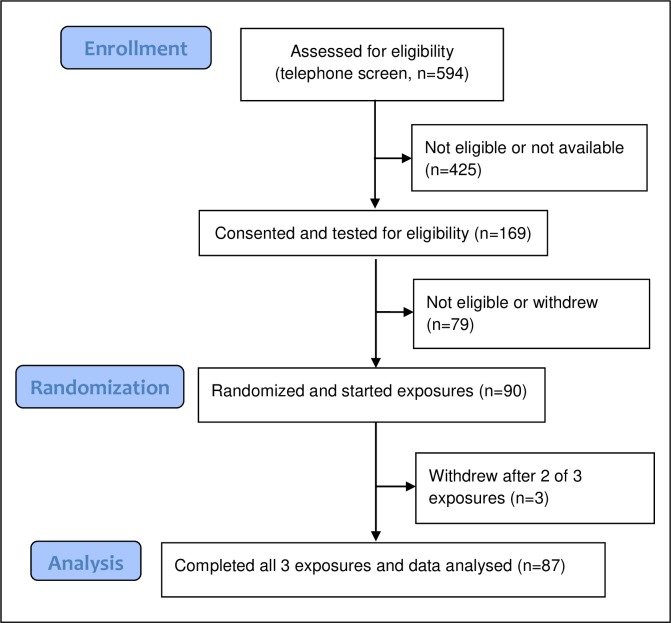
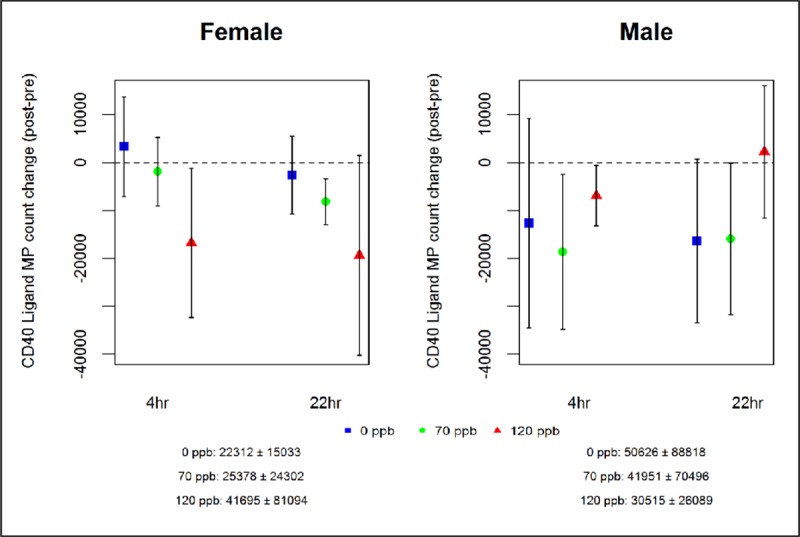
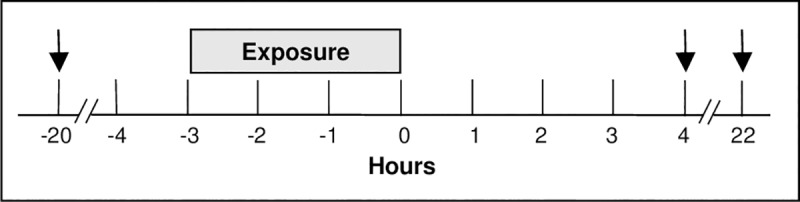
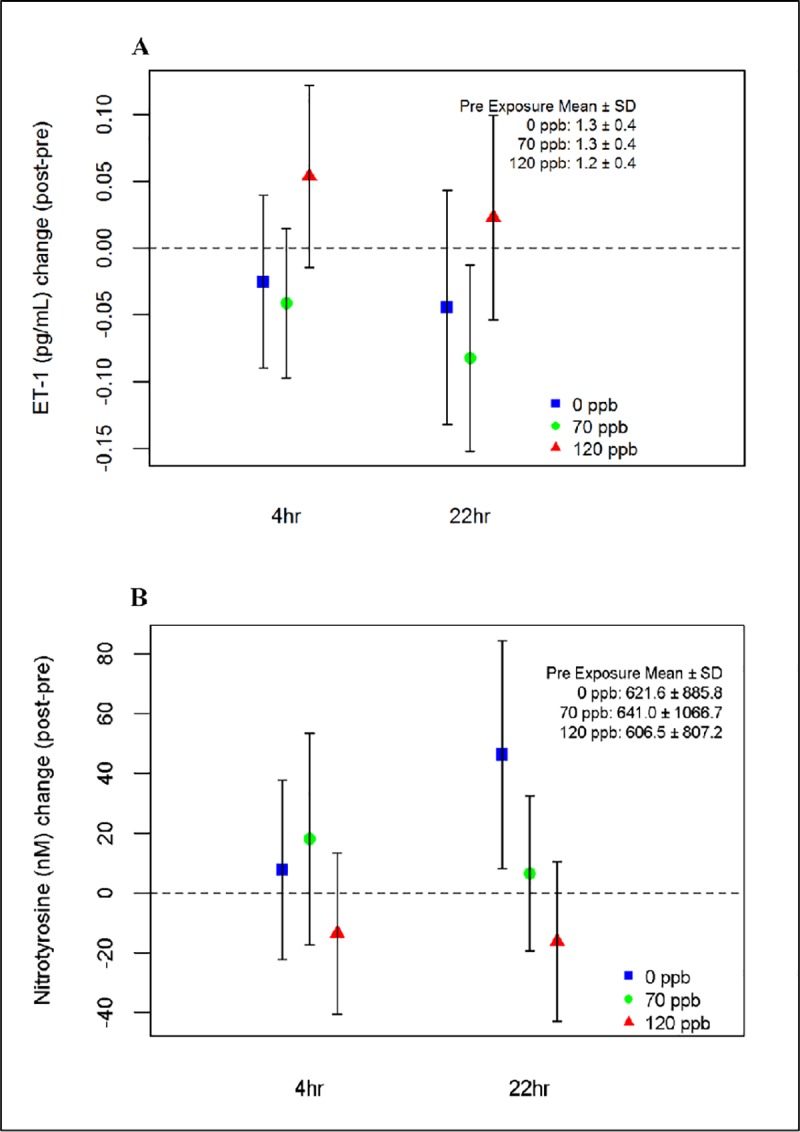
The evidence that exposure to ozone air pollution causes acute cardiovascular effects is mixed. We postulated that exposure to ambient levels of ozone would increase blood markers of systemic inflammation, prothrombotic state, oxidative stress, and vascular dysfunction in healthy older subjects, and that absence of the glutathione S-transferase Mu 1 (GSTM1) gene would confer increased susceptibility. This double-blind, randomized, crossover study of 87 healthy volunteers 55-70 years of age was conducted at three sites using a common protocol. Subjects were exposed for 3 h in random order to 0 parts per billion (ppb) (filtered air), 70 ppb, and 120 ppb ozone, alternating 15 min of moderate exercise and rest. Blood was obtained the day before, approximately 4 h after, and approximately 22 h after each exposure. Linear mixed effect and logistic regression models evaluated the impact of exposure to ozone on pre-specified primary and secondary outcomes. The definition of statistical significance was p<0.01. There were no effects of ozone on the three primary markers of systemic inflammation and a prothrombotic state: C-reactive protein, monocyte-platelet conjugates, and microparticle-associated tissue factor activity. However, among the secondary endpoints, endothelin-1, a potent vasoconstrictor, increased from pre- to post-exposure with ozone concentration (120 vs 0 ppb: 0.07 pg/mL, 95% confidence interval [CI] 0.01, 0.14; 70 vs 0 ppb: -0.03 pg/mL, CI -0.09, 0.04; p = 0.008). Nitrotyrosine, a marker of oxidative and nitrosative stress, decreased with increasing ozone concentrations, with marginal significance (120 vs 0 ppb: -41.5, CI -70.1, -12.8; 70 vs 0 ppb: -14.2, CI -42.7, 14.2; p = 0.017). GSTM1 status did not modify the effect of ozone exposure on any of the outcomes. These findings from healthy older adults fail to identify any mechanistic basis for the epidemiologically described cardiovascular effects of exposure to ozone. The findings, however, may not be applicable to adults with cardiovascular disease.
臭氧空气污染暴露会导致急性心血管效应的证据是混杂的。我们推测,在健康的老年人中,暴露于环境水平的臭氧会增加全身炎症、促血栓形成状态、氧化应激和血管功能障碍的血液标志物,而谷胱甘肽 S-转移酶 Mu 1(GSTM1)基因缺失会增加易感性。这项在三个地点进行的、使用共同方案的、87 名 55-70 岁健康志愿者的双盲、随机、交叉研究,将参与者随机暴露于 0 个部分每十亿(ppb)(过滤空气)、70ppb 和 120ppb 臭氧中,每 15 分钟交替进行适度运动和休息。在每次暴露前一天、大约暴露后 4 小时和大约 22 小时采集血液。线性混合效应和逻辑回归模型评估了臭氧暴露对预先指定的主要和次要结果的影响。统计学意义的定义为 p<0.01。臭氧对全身炎症和促血栓形成状态的三个主要标志物没有影响:C 反应蛋白、单核细胞-血小板复合物和微粒相关组织因子活性。然而,在次要终点中,内皮素-1,一种有效的血管收缩剂,随着臭氧浓度的增加而从暴露前到暴露后增加(120 与 0 ppb:0.07pg/mL,95%置信区间[CI]0.01,0.14;70 与 0 ppb:-0.03pg/mL,CI-0.09,0.04;p=0.008)。作为氧化和硝化应激的标志物的硝基酪氨酸随着臭氧浓度的增加而减少,但具有边缘显著性(120 与 0 ppb:-41.5,CI-70.1,-12.8;70 与 0 ppb:-14.2,CI-42.7,14.2;p=0.017)。GSTM1 状态并没有改变臭氧暴露对任何结果的影响。这些来自健康老年人的发现未能确定臭氧暴露在流行病学描述的心血管效应中的任何机制基础。然而,这些发现可能不适用于患有心血管疾病的成年人。