Lin I-Hung, Chen Ying-Jen, Chang Ping-Ying, Hsiao Po-Wei, Weng Tzu-Heng, Chang Yun-Hsiang
Department of Ophthalmology.
Division of Hematology/Oncology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center.
Medicine (Baltimore). 2019 Sep;98(39):e17232. doi: 10.1097/MD.0000000000017232.
To report a rare case of severe atypical hemolytic-uremic syndrome (HUS) in a patient who presented with vitreous hemorrhage and tractional retinal detachment (TRD) in both eyes. To our knowledge, this is the first reported case of atypical HUS complicated with bilateral TRD in the literature.
A 20-year-old man with atypical HUS demonstrated bilateral visual acuity of hand motion at 30 cm.
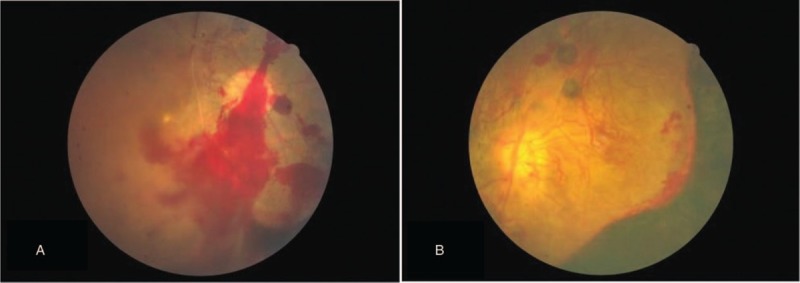
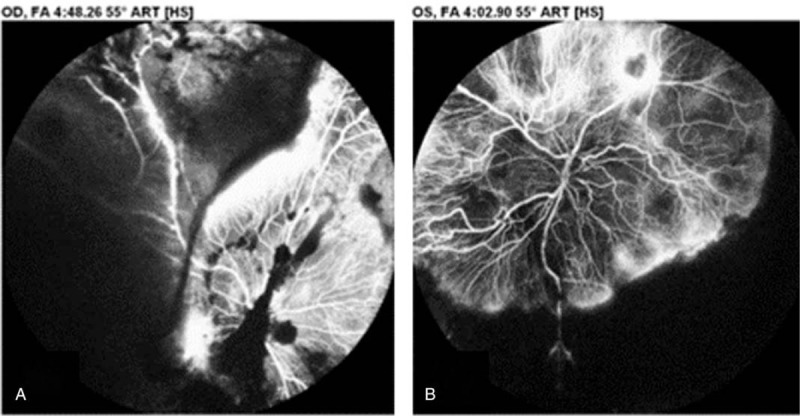
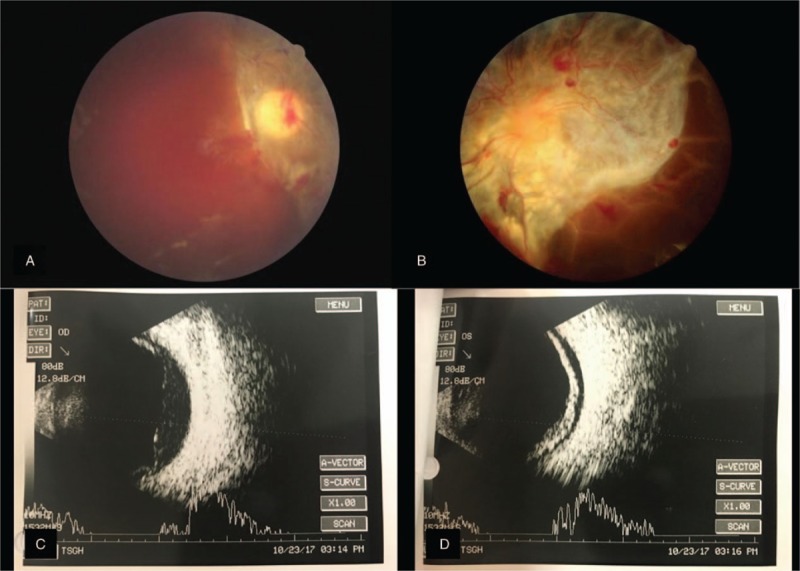
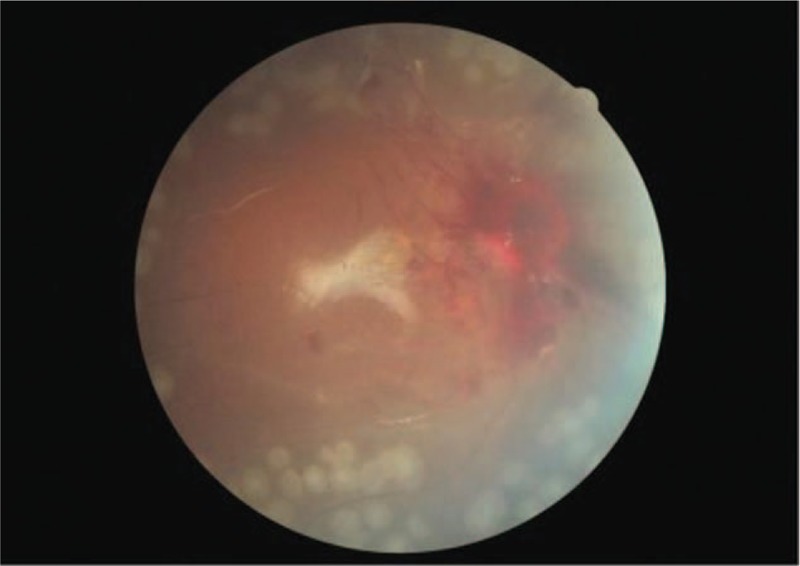
Dilated fundus examination revealed diffuse intraretinal hemorrhage with vascular engorgement, neovascularization of the disc, and neovascularization elsewhere bilaterally. Fluorescein angiography revealed bilateral proliferative retinopathy, retinal hemorrhage, and a large nonperfusion area with extensive neovascularization. Intravitreal antivascular endothelial growth factor (ranibizumab) injection was administered in both eyes, but his ophthalmic condition did not improve, and TRD developed bilaterally. Therefore atypical HUS complicated with bilateral TRD was diagnosed.
Pars plana vitrectomy was performed with panretinal photocoagulation and silicone oil tamponade in the right eye.
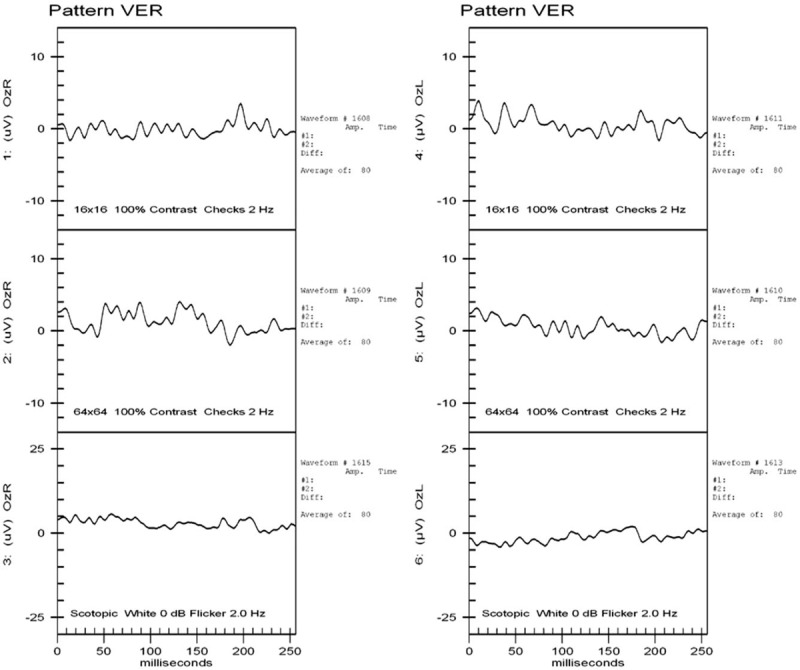
After the pars plana vitrectomy of right eye, the retina was well-attached after surgery, but visual acuity remained poor. Visual evoked potential examination showed poor waveforms bilaterally, which suggested ischemic optic neuropathy.
Atypical HUS can cause systemic thrombotic microangiopathy, resulting in ischemic retinal changes. These ischemic retinal changes can then cause hypoxia, which triggers production of angiogenic factors and subsequently causes retinal vascular hyperpermeability, retinal and vitreous neovascularization, fibrovascular proliferation, vitreous hemorrhage, and TRD, in a manner similar to that of other ischemia-induced proliferative retinopathies. Despite successful surgery in the right eye, our patient's visual acuity did not improve, possibly because of severe and generalized ischemia of intraocular tissue, which resulted in ischemic optic neuropathy.
报告1例罕见的严重非典型溶血尿毒综合征(HUS)患者,该患者双眼出现玻璃体积血和牵拉性视网膜脱离(TRD)。据我们所知,这是文献中首次报道的非典型HUS合并双侧TRD的病例。
一名20岁非典型HUS男性患者,双眼视力为30 cm处手动。
散瞳眼底检查显示双眼视网膜弥漫性出血伴血管充血、视盘新生血管形成及其他部位新生血管形成。荧光素血管造影显示双眼增殖性视网膜病变、视网膜出血以及大片无灌注区伴广泛新生血管形成。双眼均行玻璃体内抗血管内皮生长因子(雷珠单抗)注射,但眼部情况未改善,双侧出现TRD。因此诊断为非典型HUS合并双侧TRD。
右眼行玻璃体切割术联合全视网膜光凝和硅油填充。
右眼玻璃体切割术后,视网膜术后复位良好,但视力仍差。视觉诱发电位检查显示双眼波形不佳,提示缺血性视神经病变。
非典型HUS可导致全身性血栓性微血管病,引起视网膜缺血性改变。这些视网膜缺血性改变可导致缺氧,进而触发血管生成因子的产生,随后导致视网膜血管通透性增加、视网膜和玻璃体新生血管形成、纤维血管增殖、玻璃体积血和TRD,其机制与其他缺血性增殖性视网膜病变相似。尽管右眼手术成功,但患者视力未改善,可能是由于眼内组织严重广泛性缺血,导致缺血性视神经病变。