Department of Experimental and Clinical Medicine, University of Florence, Florence 50134, Italy.
Department of Biomedical, Experimental and Clinical Sciences "Mario Serio" University of Florence, Florence 50134, Italy.
World J Gastroenterol. 2019 Sep 28;25(36):5543-5558. doi: 10.3748/wjg.v25.i36.5543.
An altered (dysbiosis) and unhealthy status of the gut microbiota is usually responsible for a reduction of short chain fatty acids (SCFAs) concentration. SCFAs obtained from the carbohydrate fermentation processes are crucial in maintaining gut homeostasis and their determination in stool samples could provide a faster, reliable and cheaper method to highlight the presence of an intestinal dysbiosis and a biomarker for various gut diseases. We hypothesize that different intestinal diseases, such as celiac disease (CD), adenomatous polyposis (AP) and colorectal cancer (CRC) could display a particular fecal SCFAs' signature.
To compare the fecal SCFAs' profiles of CD, AP, CRC patients and healthy controls, using the same analytical method.
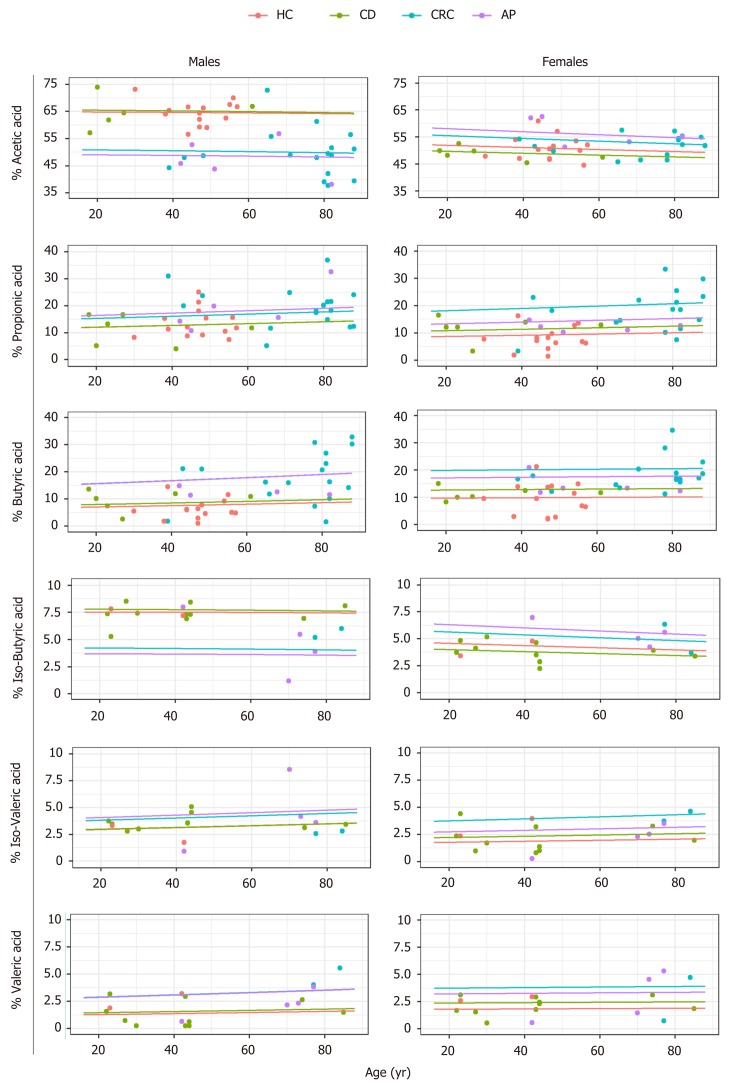
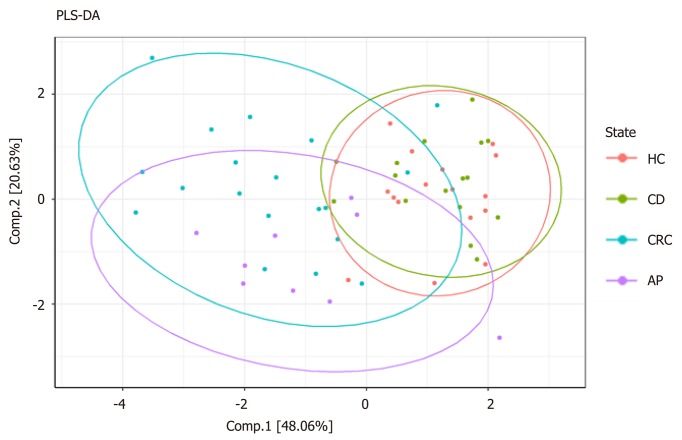
In this cross-sectional study, we defined and compared the SCFAs' concentration in fecal samples of 9 AP, 16 CD, 19 CRC patients and 16 healthy controls (HC). The SCFAs' analysis were performed using a gas-chromatography coupled with mass spectrometry method. Data analysis was carried out using Wilcoxon rank-sum test to assess pairwise differences of SCFAs' profiles, partial least squares-discriminate analysis (PLS-DA) to determine the status membership based on distinct SCFAs' profiles, and Dirichlet regression to determine factors influencing concentration levels of SCFAs.
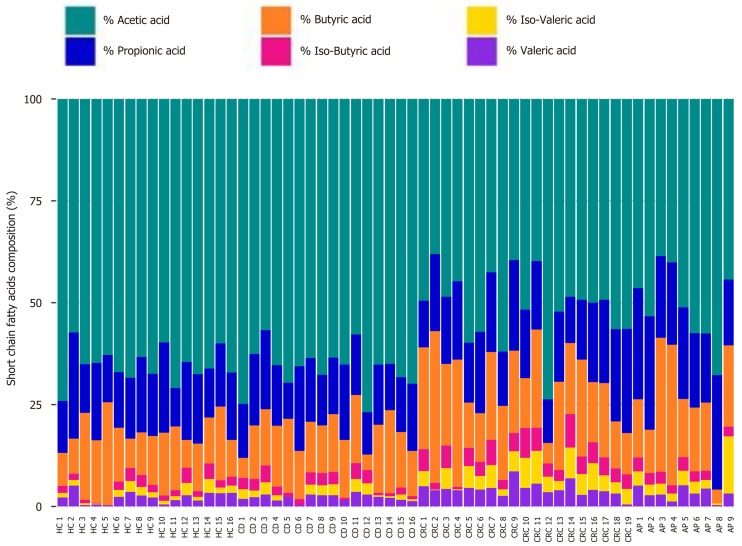
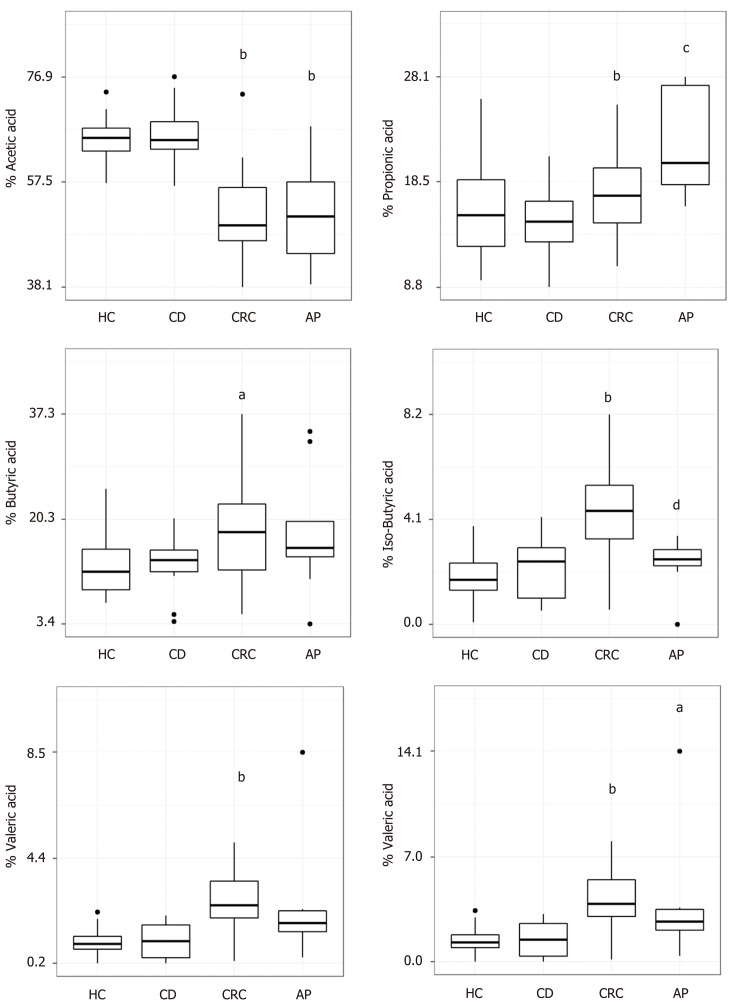
We have not observed any difference in the SCFAs' amount and composition between CD and healthy control. On the contrary, the total amount of SCFAs was significantly lower in CRC patients compared to HC ( = 0.044) and CD ( = 0.005). Moreover, the SCFAs' percentage composition was different in CRC and AP compared to HC. In detail, HC displayed higher percentage of acetic acid ( value = 1.3 × 10) and a lower amount of butyric ( value = 0.02192), isobutyric ( value = 7.4 × 10), isovaleric ( value = 0.00012) and valeric ( value = 0.00014) acids compared to CRC patients. AP showed a lower abundance of acetic acid ( value = 0.00062) and higher percentages of propionic ( value = 0.00433) and isovaleric ( value = 0.00433) acids compared to HC. Moreover, AP showed higher levels of propionic acid ( value = 0.03251) and a lower level of isobutyric acid ( value = 0.00427) in comparison to CRC. The PLS-DA model demonstrated a significant separation of CRC and AP groups from HC, although some degree of overlap was observed between CRC and AP.
Analysis of fecal SCFAs shows the potential to provide a non-invasive means of diagnosis to detect patients with CRC and AP, while CD patients cannot be discriminated from healthy subjects.
肠道微生物群落的改变(失调)和不健康状态通常会导致短链脂肪酸(SCFAs)浓度降低。碳水化合物发酵过程中产生的 SCFAs 对维持肠道内环境稳定至关重要,其在粪便样本中的测定可以提供一种更快、更可靠、更经济的方法来突出肠道菌群失调的存在,并作为各种肠道疾病的生物标志物。我们假设不同的肠道疾病,如乳糜泻(CD)、腺瘤性息肉(AP)和结直肠癌(CRC)可能具有特定的粪便 SCFAs 特征。
使用相同的分析方法比较 CD、AP、CRC 患者和健康对照者的粪便 SCFAs 谱。
在这项横断面研究中,我们定义并比较了 9 例 AP、16 例 CD、19 例 CRC 患者和 16 例健康对照者(HC)粪便样本中的 SCFAs 浓度。使用气相色谱-质谱联用方法进行 SCFAs 分析。使用 Wilcoxon 秩和检验评估 SCFAs 谱的两两差异,使用偏最小二乘判别分析(PLS-DA)根据不同的 SCFAs 谱确定状态成员,使用 Dirichlet 回归确定影响 SCFAs 浓度水平的因素。
我们没有观察到 CD 和健康对照组之间 SCFAs 数量和组成的任何差异。相反,与 HC( = 0.044)和 CD( = 0.005)相比,CRC 患者的 SCFAs 总量明显较低( = 0.044)。此外,与 HC 相比,CRC 和 AP 中的 SCFAs 百分比组成不同。具体而言,HC 显示出更高的乙酸百分比( 值 = 1.3 × 10)和更低的丁酸( 值 = 0.02192)、异丁酸( 值 = 7.4 × 10)、异戊酸( 值 = 0.00012)和戊酸( 值 = 0.00014)含量。AP 与 HC 相比,乙酸丰度较低( 值 = 0.00062),丙酸( 值 = 0.00433)和异戊酸( 值 = 0.00433)百分比较高。此外,与 CRC 相比,AP 显示出更高水平的丙酸( 值 = 0.03251)和较低水平的异丁酸( 值 = 0.00427)。PLS-DA 模型显示 CRC 和 AP 组与 HC 有显著的分离,但在 CRC 和 AP 之间观察到一定程度的重叠。
粪便 SCFAs 的分析显示出提供一种非侵入性诊断方法来检测 CRC 和 AP 患者的潜力,而 CD 患者不能与健康受试者区分开来。