Department of Gastroenterology, Kaiser Permanente San Francisco, San Francisco, California; Division of Research, Kaiser Permanente Northern California, Oakland, California.
Division of Research, Kaiser Permanente Northern California, Oakland, California.
Gastroenterology. 2020 Mar;158(4):884-894.e5. doi: 10.1053/j.gastro.2019.09.039. Epub 2019 Oct 4.
BACKGROUND & AIMS: The long-term risks of colorectal cancer (CRC) and CRC-related death following adenoma removal are uncertain. Data are needed to inform evidence-based surveillance guidelines, which vary in follow-up recommendations for some polyp types. Using data from a large, community-based integrated health care setting, we examined the risks of CRC and related death by baseline colonoscopy adenoma findings.
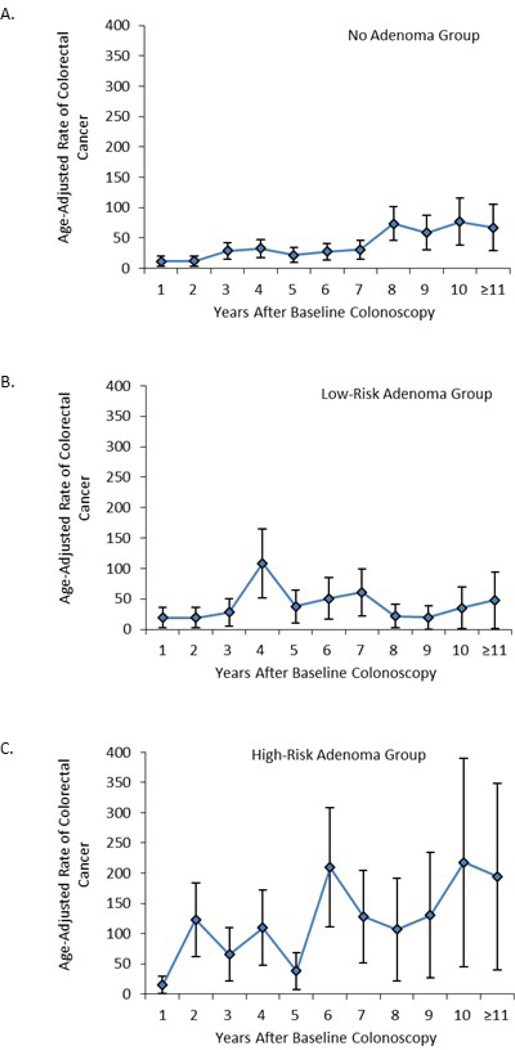
Participants at 21 medical centers underwent baseline colonoscopies from 2004 through 2010; findings were categorized as no-adenoma, low-risk adenoma, or high-risk adenoma. Participants were followed until the earliest of CRC diagnosis, death, health plan disenrollment, or December 31, 2017. Risks of CRC and related deaths among the high- and low-risk adenoma groups were compared with the no-adenoma group using Cox regression adjusting for confounders.
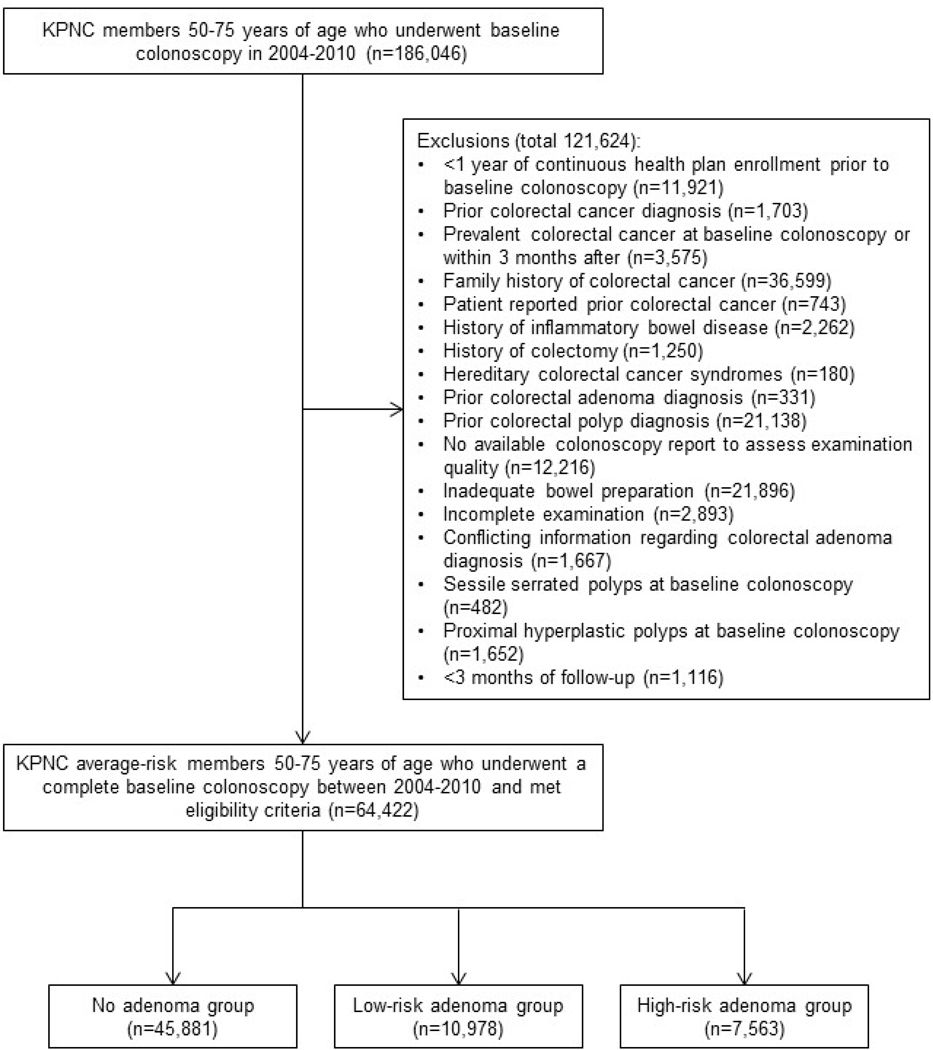
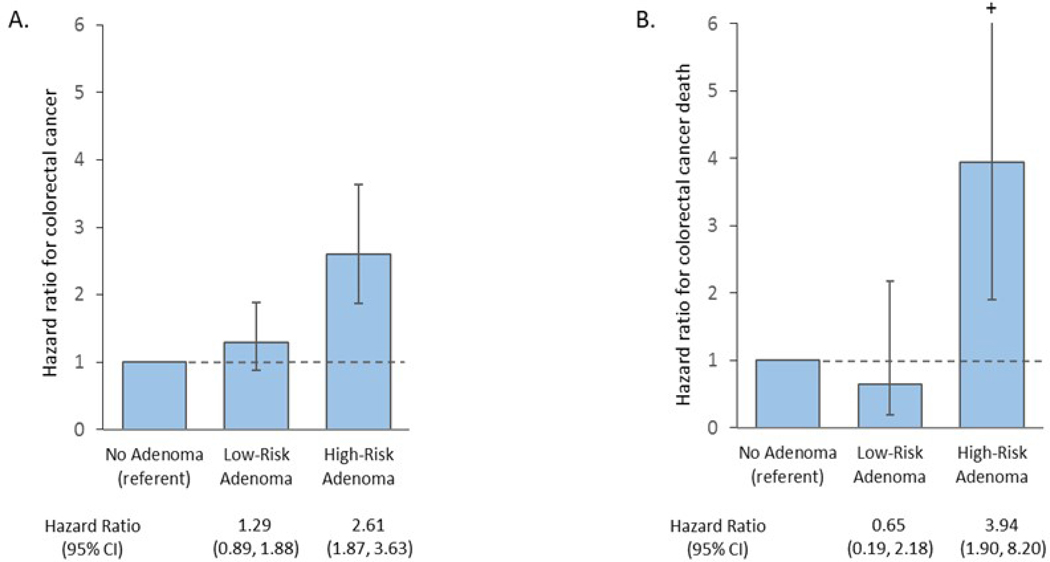
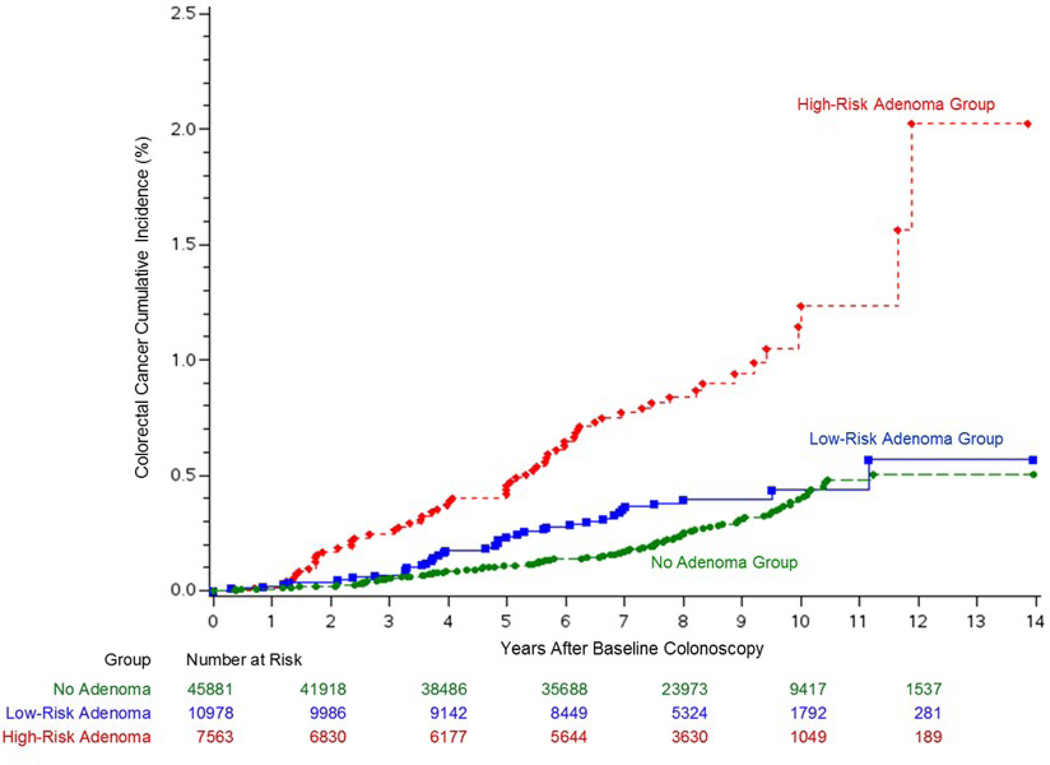
Among 186,046 patients, 64,422 met eligibility criteria (54.3% female; mean age, 61.6 ± 7.1 years; median follow-up time, 8.1 years from the baseline colonoscopy). Compared with the no-adenoma group (45,881 patients), the high-risk adenoma group (7563 patients) had a higher risk of CRC (hazard ratio [HR] 2.61; 95% confidence interval [CI] 1.87-3.63) and related death (HR 3.94; 95% CI 1.90-6.56), whereas the low-risk adenoma group (10,978 patients) did not have a significant increase in risk of CRC (HR 1.29; 95% CI 0.89-1.88) or related death (HR 0.65; 95% CI 0.19-2.18).
With up to 14 years of follow-up, high-risk adenomas were associated with an increased risk of CRC and related death, supporting early colonoscopy surveillance. Low-risk adenomas were not associated with a significantly increased risk of CRC or related deaths. These results can inform current surveillance guidelines for high- and low-risk adenomas.
腺瘤切除术后结直肠癌(CRC)和 CRC 相关死亡的长期风险尚不确定。需要数据来为循证监测指南提供信息,这些指南对某些息肉类型的随访建议存在差异。本研究使用来自大型社区综合医疗保健环境的数据,根据基线结肠镜检查腺瘤发现结果,检查 CRC 和相关死亡的风险。
21 家医疗中心的参与者在 2004 年至 2010 年期间进行了基线结肠镜检查;结果分为无腺瘤、低危腺瘤或高危腺瘤。参与者的随访时间最早为 CRC 诊断、死亡、健康计划退出或 2017 年 12 月 31 日。使用 Cox 回归校正混杂因素后,比较高危腺瘤组和低危腺瘤组与无腺瘤组的 CRC 和相关死亡风险。
在 186046 名患者中,64422 名符合入选标准(54.3%为女性;平均年龄 61.6±7.1 岁;从基线结肠镜检查开始的中位随访时间为 8.1 年)。与无腺瘤组(45881 名患者)相比,高危腺瘤组(7563 名患者)CRC 的风险更高(风险比 [HR] 2.61;95%置信区间 [CI] 1.87-3.63)和相关死亡(HR 3.94;95% CI 1.90-6.56),而低危腺瘤组(10978 名患者)CRC(HR 1.29;95% CI 0.89-1.88)或相关死亡(HR 0.65;95% CI 0.19-2.18)的风险无显著增加。
在长达 14 年的随访中,高危腺瘤与 CRC 和相关死亡风险增加相关,支持早期结肠镜监测。低危腺瘤与 CRC 或相关死亡风险的显著增加无关。这些结果可以为高风险和低风险腺瘤的现行监测指南提供信息。