Center for Health Decision Science, Harvard T.H. Chan School of Public Health, Boston, Massachusetts.
Comparative Health Outcomes, Policy, and Economics Institute, University of Washington, Seattle.
JAMA Netw Open. 2019 Oct 2;2(10):e1912925. doi: 10.1001/jamanetworkopen.2019.12925.
Eating disorders (EDs) are common psychiatric disorders associated with high mortality. However, data on ED disease dynamics and treatment coverage are sparse.
To model the individual-level disease dynamics of ED from birth to age 40 years and to estimate the association of increased treatment coverage with ED-related mortality.
DESIGN, SETTING, AND PARTICIPANTS: In this decision analytical model study, an individual-level Markov state transition model was empirically calibrated in April 2019 using a Bayesian approach to synthesize available clinical and epidemiologic ED data. The simulation model was calibrated to nationally representative US survey data from 2007 and 2011. A virtual cohort of 100 000 individuals (50 000 [50%] male) was modeled from birth to age 40 years for 4 ED diagnoses: anorexia nervosa, bulimia nervosa, binge eating disorder, and other specified feeding and eating disorders.
Age-specific ED incidence and mortality rates and background (all-cause) mortality.
The main outcomes were age-specific 12-month and lifetime ED prevalence and number of deaths per 100 000 general population individuals by age 40 years. The mean and 95% uncertainty intervals (UIs) of 1000 simulations, accounting for stochastic and parameter uncertainty, are reported.
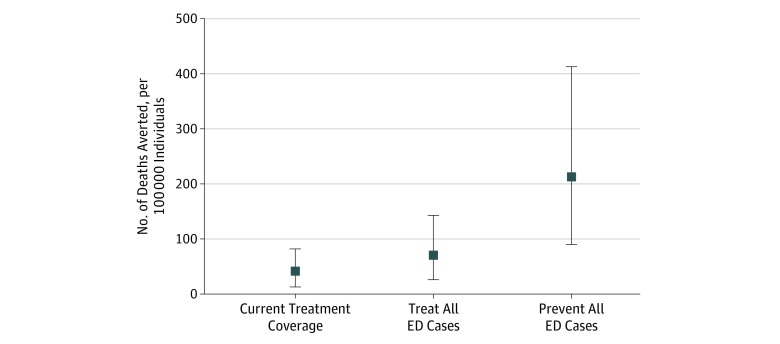
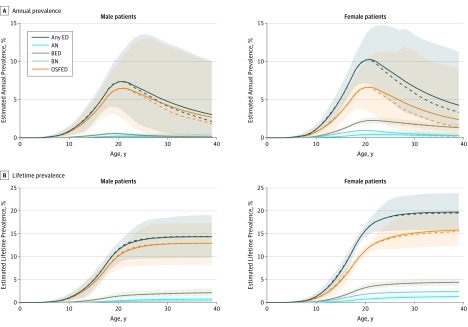
The highest estimated mean annual prevalence of ED occurred at approximately age 21 years for both male individuals (7.4%; 95% UI, 3.5%-11.5%) and female individuals (10.3%; 95% UI, 7.0%-14.2%), with lifetime mean prevalence estimates increasing to 14.3% (95% UI, 9.7%-19.0%) for male individuals and 19.7% (95% UI, 15.8%-23.9%) for female individuals by age 40 years. Ninety-five percent of first-time cases occurred by age 25 years. Current treatment coverage averts an estimated mean of 41.7 deaths per 100 000 people (95% UI, 13.0-82.0 deaths per 100 000 people) by age 40 years, whereas increasing treatment coverage for all patients with ED could avert an estimated mean of 70.5 deaths per 100 000 people by age 40 years (95% UI, 26.0-143.0 deaths per 100 000 people).
In this simulation modeling study, the estimated lifetime prevalence of ED was high, with approximately 1 in 7 male and 1 in 5 female individuals having an ED by age 40 years. The initial onset of EDs was highly concentrated during adolescence and young adulthood, suggesting that this is a critical period for prevention efforts. However, the high estimated prevalence of recurring ED later in life highlights the importance of identification and treatment of ED at older ages as well. These findings suggest that increasing treatment coverage could substantially reduce ED-related mortality.
饮食失调(ED)是一种常见的精神疾病,与高死亡率有关。然而,关于 ED 疾病动态和治疗覆盖率的数据很少。
从出生到 40 岁的个体水平上建模 ED 的疾病动态,并估计增加治疗覆盖率与 ED 相关死亡率的关系。
设计、设置和参与者:在这项决策分析模型研究中,使用贝叶斯方法在 2019 年 4 月对一个经验性校准的个体水平马尔可夫状态转移模型进行了实证校准,以综合现有的临床和流行病学 ED 数据。该仿真模型根据 2007 年和 2011 年的全国代表性美国调查数据进行了校准。从出生到 40 岁,对 10 万名个体(5 万名男性[50%])的 4 种 ED 诊断(神经性厌食症、神经性贪食症、暴食障碍和其他特定的喂养和进食障碍)进行了虚拟队列建模。
特定年龄的 ED 发病率和死亡率以及背景(全因)死亡率。
主要结果是特定年龄的 12 个月和终生 ED 患病率以及到 40 岁时每 10 万名普通人群中死亡人数。报告了 1000 次模拟的平均值和 95%置信区间(UI),以考虑随机和参数不确定性。
男性个体(7.4%;95%UI,3.5%-11.5%)和女性个体(10.3%;95%UI,7.0%-14.2%)在大约 21 岁时估计的 ED 年平均患病率最高,到 40 岁时终生患病率估计值分别增加到男性个体的 14.3%(95%UI,9.7%-19.0%)和女性个体的 19.7%(95%UI,15.8%-23.9%)。95%的首次发病发生在 25 岁之前。目前的治疗覆盖率可以避免到 40 岁时估计平均 41.7 人死亡(95%UI,13.0-82.0 人死亡),而增加所有 ED 患者的治疗覆盖率可以避免到 40 岁时估计平均 70.5 人死亡(95%UI,26.0-143.0 人死亡)。
在这项模拟建模研究中,ED 的终生患病率估计很高,大约有 1/7 的男性和 1/5 的女性到 40 岁时患有 ED。ED 的初始发病高度集中在青少年和成年早期,这表明这是预防工作的关键时期。然而,晚年 ED 反复发作的高估计患病率突出表明,在老年识别和治疗 ED 也很重要。这些发现表明,增加治疗覆盖率可以大大降低 ED 相关死亡率。