Johns Hopkins University, Bloomberg School of Public Health, Department of International Health, Institute for International Programs, Baltimore, Maryland, USA.
World Health Organization, Department of Maternal, Newborn, Child and Adolescent Health Child and Adolescent Health and Development, Geneva, Switzerland.
J Glob Health. 2019 Dec;9(2):020801. doi: 10.7189/jogh.09.020801.
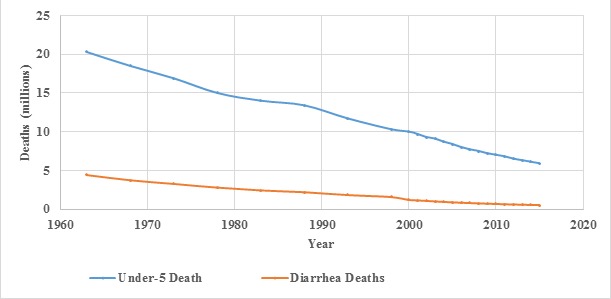
Childhood diarrhea deaths have declined more than 80% from 1980 to 2015, in spite of an increase in the number of children in low- and middle-income countries (LMIC). Possible drivers of this remarkable accomplishment can guide the further reduction of the half million annual child deaths from diarrhea that still occur.
We used the Lives Saved Tool, which models effects on mortality due to changes in coverage of preventive or therapeutic interventions or risk factors, for 50 LMIC to determine the proximal drivers of the diarrhea mortality reduction.
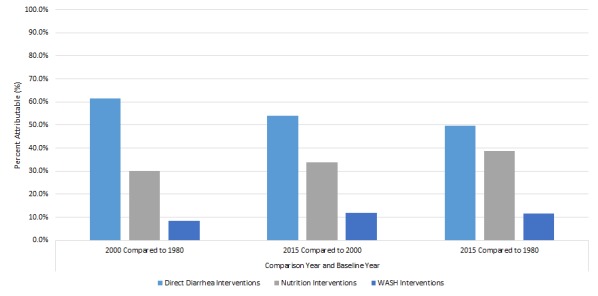
Diarrhea treatment (oral rehydration solution [ORS], zinc, antibiotics for dysentery and management of persistent diarrhea) and use of rotavirus vaccine accounted for 49.7% of the diarrhea mortality reduction from 1980 to 2015. Improvements in nutrition (stunting, wasting, breastfeeding practices, vitamin A) accounted for 38.8% and improvements in water, sanitation and handwashing for 11.5%. The contribution of ORS was greater from 1980 to 2000 (58.0% of the reduction) than from 2000 to 2015 (30.7%); coverage of ORS increased from zero in 1980 to 29.5% in 2000 and more slowly to 44.1% by 2015. To eliminate the remaining childhood diarrhea deaths globally, all these interventions will be needed. Scaling up diarrhea treatment and rotavirus vaccine, to 90% coverage could reduce global child diarrhea mortality by 74.1% from 2015 levels by 2030. Adding improved nutrition could increase that to 89.1%. Finally, adding increased use of improved water sources, sanitation and handwashing could result in a 92.8% reduction from the 2015 level.
Employing the interventions that have resulted in such a large reduction in diarrhea mortality in the last 35 years can virtually eliminate remaining childhood diarrhea deaths by 2030.
尽管中低收入国家(LMIC)的儿童数量有所增加,但自 1980 年至 2015 年,儿童腹泻死亡人数已减少 80%以上。这一显著成就的可能驱动因素可以为进一步减少每年仍有 50 万死于腹泻的儿童提供指导。
我们使用 Lives Saved Tool,该工具模型可以针对预防或治疗干预措施或风险因素覆盖率的变化对死亡率产生的影响,对 50 个中低收入国家进行分析,以确定腹泻死亡率降低的近端驱动因素。
腹泻治疗(口服补液盐[ORS]、锌、痢疾抗生素和持续性腹泻管理)和轮状病毒疫苗的使用占 1980 年至 2015 年腹泻死亡率降低的 49.7%。营养改善(发育迟缓、消瘦、母乳喂养做法、维生素 A)占 38.8%,水、环境卫生和手卫生改善占 11.5%。从 1980 年到 2000 年,ORS 的贡献更大(减少的 58.0%),而从 2000 年到 2015 年,ORS 的贡献更小(减少的 30.7%);ORS 的覆盖率从 1980 年的零增加到 2000 年的 29.5%,到 2015 年增长速度较慢,仅达到 44.1%。为了在全球范围内消除剩余的儿童腹泻死亡,所有这些干预措施都将是必要的。将腹泻治疗和轮状病毒疫苗的覆盖率扩大到 90%,到 2030 年可将全球儿童腹泻死亡率从 2015 年的水平降低 74.1%。添加改善营养可将这一比例提高到 89.1%。最后,增加使用改良水源、环境卫生和手卫生可使 2015 年的水平降低 92.8%。
在过去 35 年中,采用这些干预措施已使腹泻死亡率大幅降低,到 2030 年几乎可以消除剩余的儿童腹泻死亡。