Department of Anaesthesiology and Intensive Care Medicine, University Hospital Tübingen, Eberhard-Karls-University Tübingen, Hoppe-Seyler-Str. 3, 72076, Tübingen, Germany.
Department of Anesthesia and Intensive Care Medicine, Klinikum Ingolstadt, Krumenauerstr. 25, 85049, Ingolstadt, Germany.
BMC Anesthesiol. 2019 Nov 4;19(1):199. doi: 10.1186/s12871-019-0870-z.
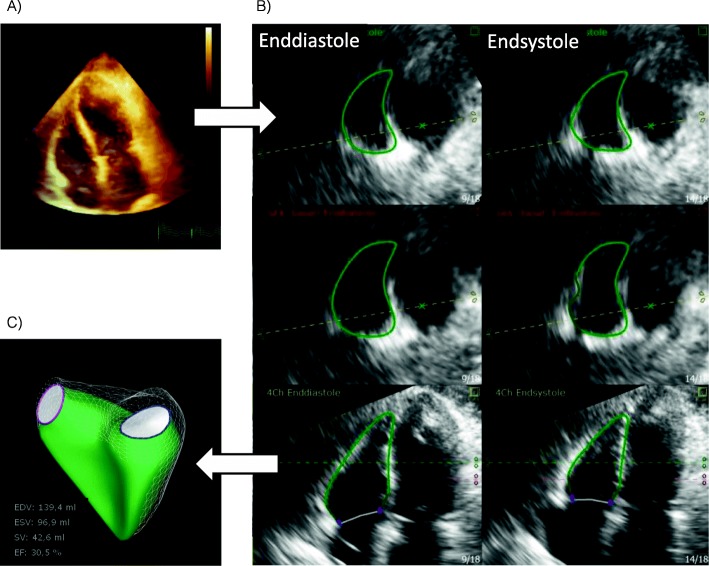
General anesthesia induction with the initiation of positive pressure ventilation creates a vulnerable phase for patients. The impact of positive intrathoracic pressure on cardiac performance has been studied but remains controversial. 3D echocardiography is a valid and MRI-validated bed-side tool to evaluate the right ventricle (RV). The aim of this study was to assess the impact of anesthesia induction (using midazolam, sufentanil and rocuronium, followed by sevoflurane) with positive pressure ventilation (PEEP 5, tidal volume 6-8 ml/kg) on 2D and 3D echocardiography derived parameters of RV function.
A prospective observational study on fifty-three patients undergoing elective cardiac surgery in a tertiary care university hospital was designed. Transthoracic echocardiography exams were performed before and immediately after anesthesia induction and were recorded together with hemodynamic parameters and ventilator settings.
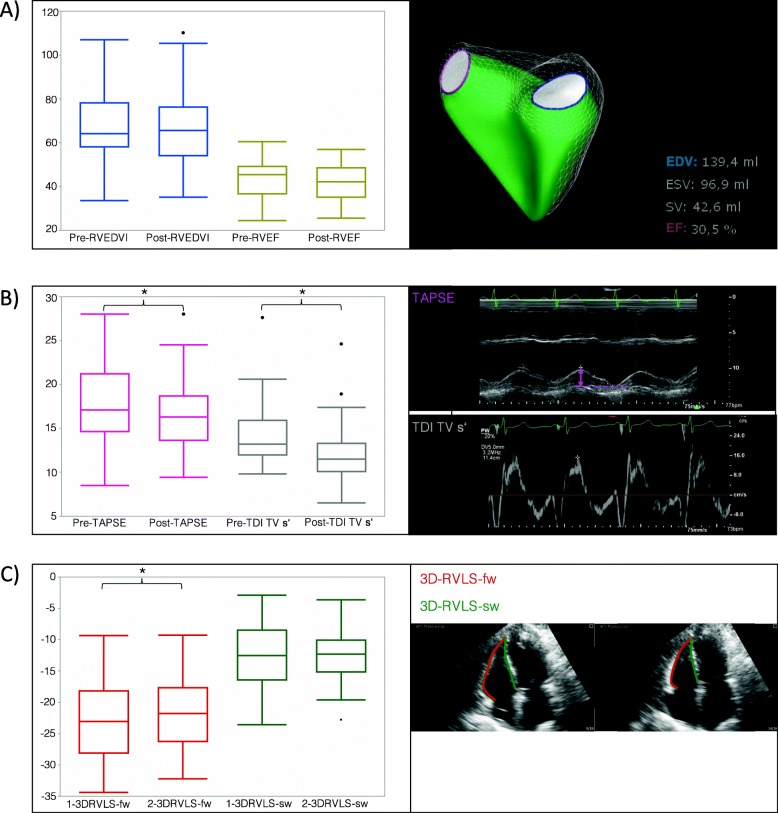
After anesthesia induction TAPSE (mean difference - 1.6 mm (95% CI - 2.6 mm to - 0.7 mm; p = 0.0013) as well as the Tissue Doppler derived tricuspid annulus peak velocity (TDITVs') were significantly reduced (mean difference - 1.9% (95% CI: - 2.6 to - 1.2; p < 0.0001), but global right ventricular ejection fraction (RVEF; p = 0.1607) and right ventricular stroke volume (RVSV; p = 0.1838) did not change.
This data shows a preserved right ventricular ejection fraction and right ventricular stroke volume after anesthesia induction and initiation of positive pressure ventilation. However, the baso-apical right ventricular function is significantly reduced. Larger studies are needed in order to determine the clinical impact of these findings especially in patients presenting with impaired right ventricular function before anesthesia induction.
Retrospecitvely registered, 6th June 2016, ClinicalTrials.gov Identifier NCT02820727 .
全身麻醉诱导并开始正压通气会使患者处于脆弱阶段。正压通气对心功能的影响已被研究,但仍存在争议。三维超声心动图是一种有效的、经 MRI 验证的床边工具,可用于评估右心室(RV)。本研究旨在评估麻醉诱导(使用咪达唑仑、舒芬太尼和罗库溴铵,随后使用七氟醚)和正压通气(PEEP 为 5,潮气量为 6-8ml/kg)对 2D 和 3D 超声心动图衍生的 RV 功能参数的影响。
设计了一项在三级护理大学医院接受择期心脏手术的 53 例患者的前瞻性观察性研究。在麻醉诱导前和麻醉诱导后立即进行经胸超声心动图检查,并与血流动力学参数和呼吸机设置一起记录。
麻醉诱导后,TAPSE(平均差异-1.6mm(95%CI-2.6mm 至-0.7mm;p=0.0013)和组织多普勒衍生三尖瓣环峰值速度(TDITVs')显著降低(平均差异-1.9%(95%CI:-2.6 至-1.2;p<0.0001),但整体右心室射血分数(RVEF;p=0.1607)和右心室每搏量(RVSV;p=0.1838)无变化。
这些数据显示,在麻醉诱导和正压通气开始后,右心室射血分数和右心室每搏量保持不变,但基底-顶部右心室功能显著降低。需要更大的研究来确定这些发现的临床意义,特别是在麻醉诱导前存在右心室功能受损的患者中。
回顾性注册,2016 年 6 月 6 日,ClinicalTrials.gov 标识符 NCT02820727。