Hoosen Koraisha, Mosam Anisa, Dlova Ncoza Cordelia, Grayson Wayne
Department of Dermatology, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa.
Division of Anatomical Pathology, School of Pathology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Dermatopathology (Basel). 2019 Jun 26;6(2):111-125. doi: 10.1159/000496389. eCollection 2019 Apr-Jun.
The global mortality from HIV and the cutaneous burden of infective, inflammatory and malignant diseases in the setting of AIDS have significantly declined following the advent of highly active antiretroviral therapy. Regrettably, there has been a contemporaneous escalation in the incidence of adverse cutaneous drug reactions (ACDR), with studies attesting that HIV-positive individuals are a hundred times more susceptible to drug reactions than the general population, and advanced immunodeficiency portending an even greater risk. Several variables are accountable for this amplified risk in HIV.
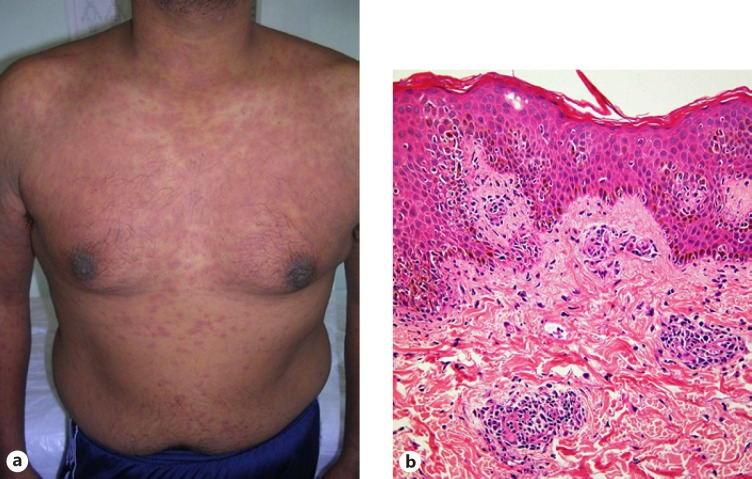
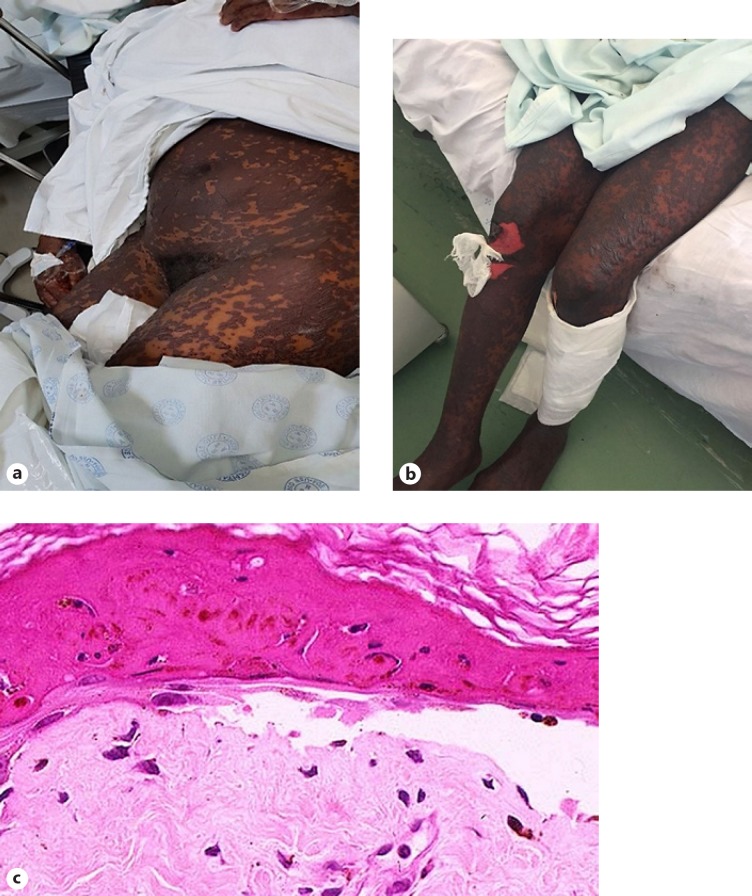
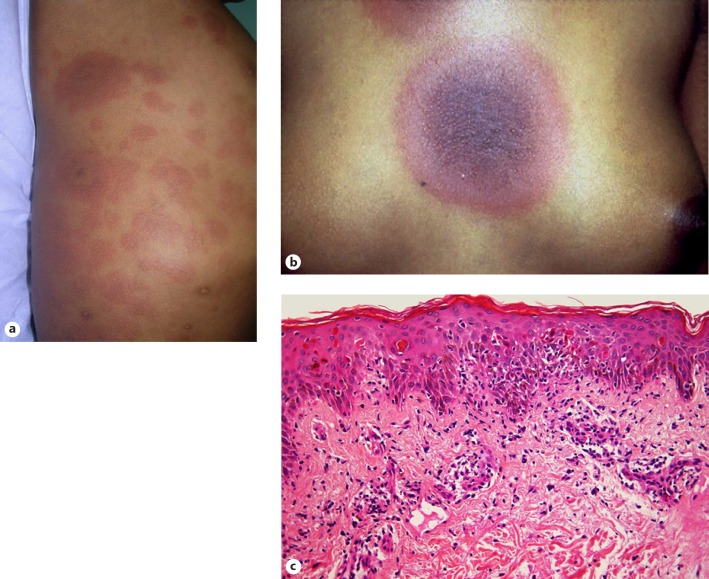
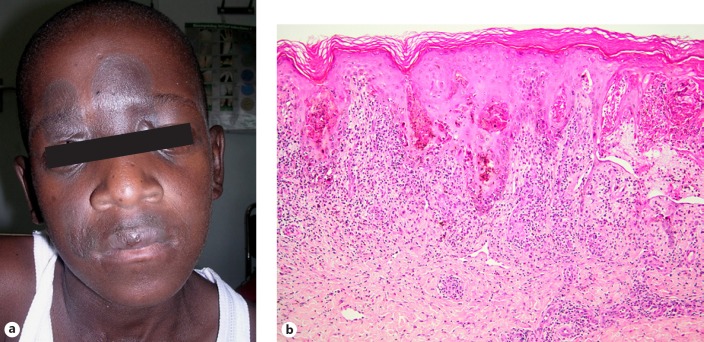
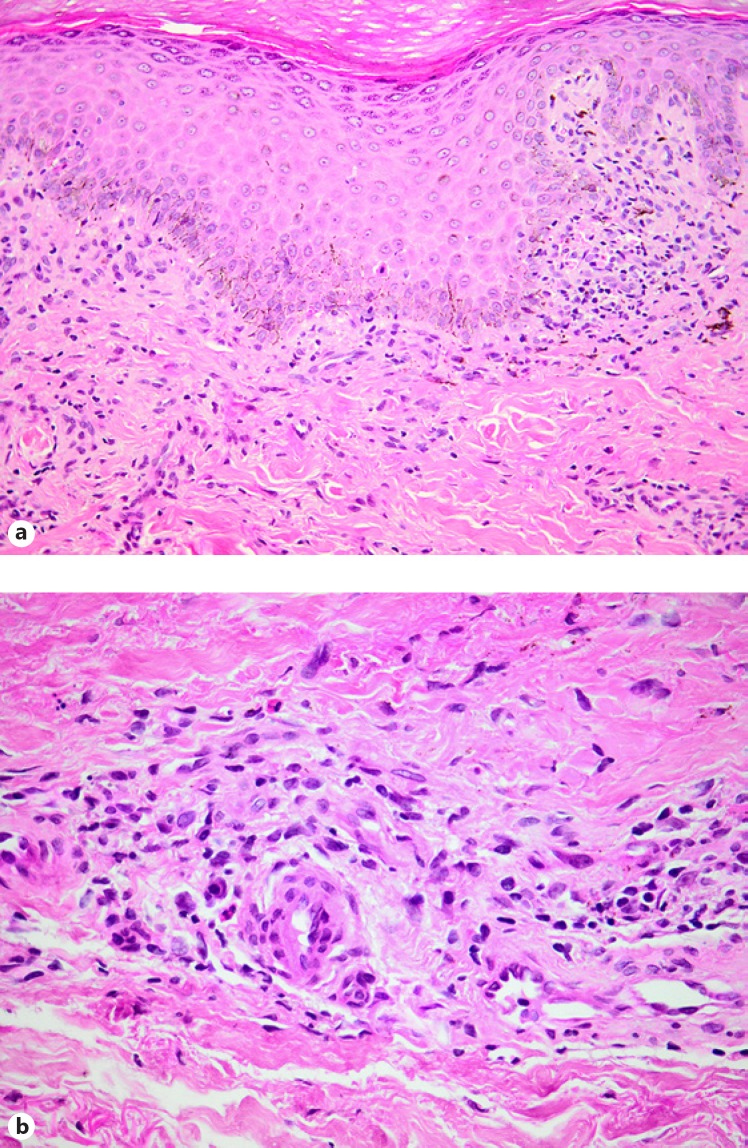
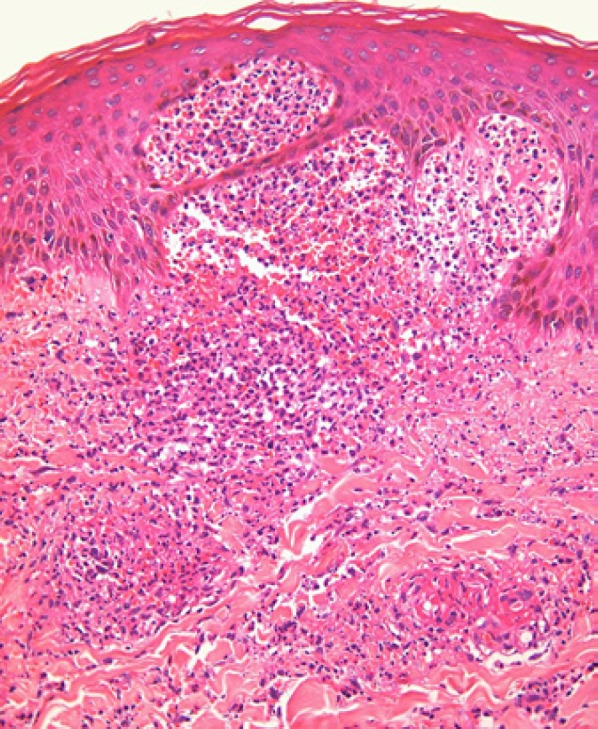
Adverse reactions to trimethoprim-sulfamethoxazole are the most common, increasing from approximately 2-8% in the general population over to 43% amongst HIV-positive individuals to approximately 69% in subjects with AIDS. Antituberculosis drugs and antiretrovirals are also well-known instigators of ACDR. Cutaneous reactions range from mild morbilliform eruptions to severe, life-threatening manifestations in the form of Stevens-Johnson syndrome/toxic epidermal necrolysis. Histological features vary from vacuolar interface changes to full-thickness epidermal necrosis with subepidermal blister formation. A precipitous diagnosis of the ACDR, clinically and histologically if necessary, together with the isolation of the causative drug is critical. The identification process, however, is often complex and multifaceted due to polypharmacy and inconclusive data on which drugs are the most likely offending agents, especially against the background of tuberculosis co-infection.
Whilst milder cutaneous reactions are treated symptomatically, severe reactions mandate immediate treatment discontinuation without rechallenge. Further studies are required to establish safe rechallenge guidelines in resource-limited settings with a high HIV and tuberculosis prevalence.
高效抗逆转录病毒疗法出现后,全球艾滋病相关的HIV死亡率以及感染性、炎症性和恶性疾病的皮肤负担显著下降。遗憾的是,与此同时,药物性皮肤不良反应(ACDR)的发生率却在上升,研究表明,HIV阳性个体发生药物反应的易感性比普通人群高百倍,而严重免疫缺陷者的风险更高。HIV感染人群中这种风险增加有几个变量可以解释。
甲氧苄啶-磺胺甲恶唑的不良反应最为常见,在普通人群中的发生率约为2%-8%,在HIV阳性个体中升至43%,在艾滋病患者中约为69%。抗结核药物和抗逆转录病毒药物也是引起ACDR的常见原因。皮肤反应范围从轻度麻疹样皮疹到严重的、危及生命的史蒂文斯-约翰逊综合征/中毒性表皮坏死松解症。组织学特征从空泡界面改变到全层表皮坏死伴表皮下疱形成。必要时从临床和组织学上迅速诊断ACDR,并找出致病药物至关重要。然而,由于联合用药以及关于哪些药物最可能是致病因素的数据尚无定论,尤其是在合并结核感染的情况下,识别过程往往复杂且涉及多方面。
轻度皮肤反应进行对症治疗,而严重反应则必须立即停药且不再重新用药。在HIV和结核病高流行的资源有限环境中,需要进一步研究以制定安全的重新用药指南。