Department of Health Management, University of Prince Edward Island, Charlottetown, Prince Edward Island, Canada.
Department of Community Health and Epidemiology, College of Medicine, University of Saskatchewan, Saskatoon, Saskatchewan, Canada.
Int J Equity Health. 2019 Nov 10;18(1):171. doi: 10.1186/s12939-019-1074-3.
A small proportion of the population consumes the majority of health care resources. High-cost health care users are a heterogeneous group. We aim to segment a provincial population into relevant homogenous sub-groups to provide actionable information on risk factors associated with high-cost health care use within sub-populations.
The Canadian Institute for Health Information (CIHI) Population Grouping methodology was used to define mutually exclusive and clinically relevant health profile sub-groups. High-cost users (> = 90th percentile of health care spending) were defined within each sub-group. Univariate analyses explored demographic, socio-economic status, health status and health care utilization variables associated with high-cost use. Multivariable logistic regression models were constructed for the costliest health profile groups.
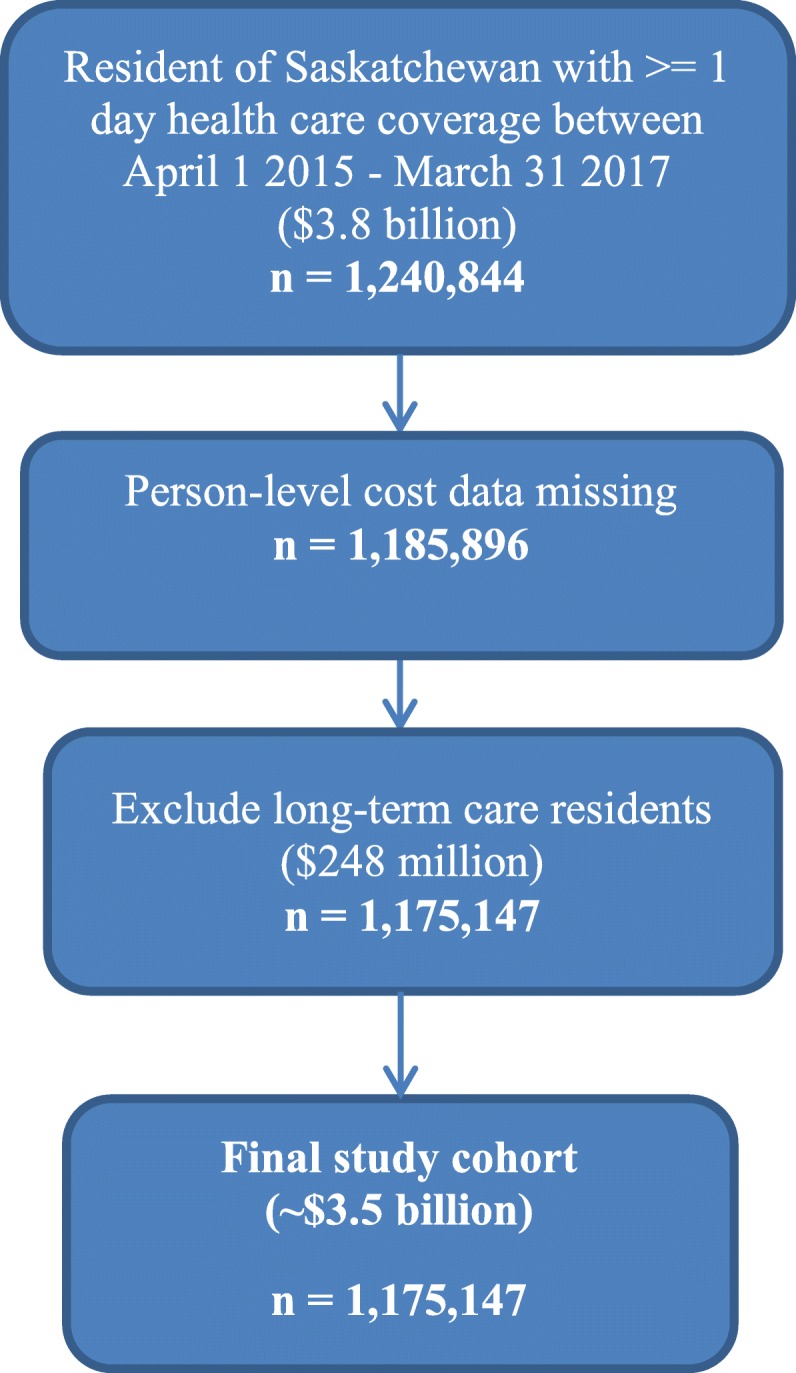
From 2015 to 2017, 1,175,147 individuals were identified for study. High-cost users consumed 41% of total health care resources. Average annual health care spending for individuals not high-cost were $642; high-cost users were $16,316. The costliest health profile groups were 'long-term care', 'palliative', 'major acute', 'major chronic', 'major cancer', 'major newborn', 'major mental health' and 'moderate chronic'. Both 'major acute' and 'major cancer' health profile groups were largely explained by measures of health care utilization and multi-morbidity. In the remaining costliest health profile groups modelled, 'major chronic', 'moderate chronic', 'major newborn' and 'other mental health', a measure of socio-economic status, low neighbourhood income, was statistically significantly associated with high-cost use.
Model results point to specific, actionable information within clinically meaningful subgroups to reduce high-cost health care use. Health equity, specifically low socio-economic status, was statistically significantly associated with high-cost use in the majority of health profile sub-groups. Population segmentation methods, and more specifically, the CIHI Population Grouping Methodology, provide specificity to high-cost health care use; informing interventions aimed at reducing health care costs and improving population health.
一小部分人口消耗了大部分医疗资源。高成本医疗保健使用者是一个异质群体。我们的目标是将省级人口划分为相关的同质亚组,为亚人群中与高成本医疗保健使用相关的风险因素提供可操作的信息。
使用加拿大健康信息研究所(CIHI)人群分组方法来定义相互排斥且具有临床相关性的健康特征亚组。在每个亚组内定义高成本使用者(> = 医疗支出第 90 百分位)。单变量分析探讨了与高成本使用相关的人口统计学、社会经济地位、健康状况和医疗保健利用变量。为最昂贵的健康特征组构建多变量逻辑回归模型。
2015 年至 2017 年,共确定了 1175147 人进行研究。高成本使用者消耗了 41%的总医疗资源。非高成本使用者的人均年医疗保健支出为 642 美元;高成本使用者为 16316 美元。最昂贵的健康特征组是“长期护理”、“姑息治疗”、“主要急性”、“主要慢性”、“主要癌症”、“主要新生儿”、“主要心理健康”和“中度慢性”。“主要急性”和“主要癌症”健康特征组主要由医疗保健利用和多疾病解释。在所建模的其余最昂贵的健康特征组中,“主要慢性”、“中度慢性”、“主要新生儿”和“其他心理健康”,社会经济地位衡量指标、低社区收入与高成本使用呈统计学显著相关。
模型结果指向具有临床意义的亚组内的具体、可操作的信息,以减少高成本医疗保健的使用。健康公平,特别是社会经济地位较低,与大多数健康特征亚组中的高成本使用呈统计学显著相关。人口细分方法,特别是 CIHI 人群分组方法,为高成本医疗保健使用提供了具体信息;为旨在降低医疗保健成本和改善人口健康的干预措施提供信息。