Lee Ching-Chi, Lee Chung-Hsun, Chen Po-Lin, Hsieh Chih-Chia, Tang Hung-Jen, Ko Wen-Chien
Graduate Institute of Medical Sciences, College of Health Sciences, Chang Jung Christian University, Tainan 71101, Taiwan.
Department of Adult Critical Care Medicine, Tainan Sin-Lau Hospital, Tainan 70142, Taiwan.
Antibiotics (Basel). 2019 Nov 10;8(4):216. doi: 10.3390/antibiotics8040216.
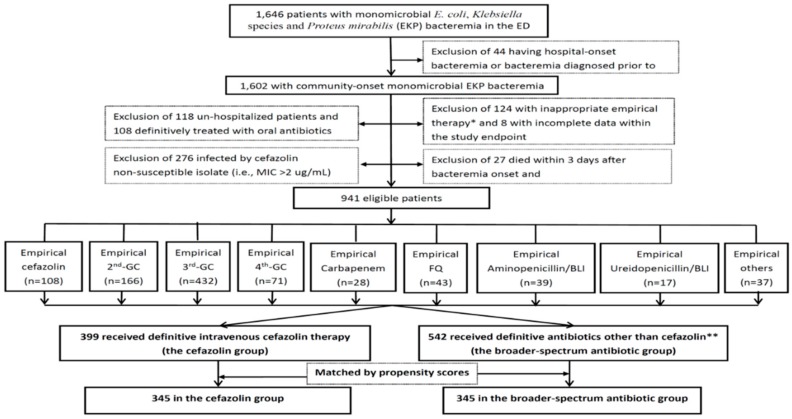
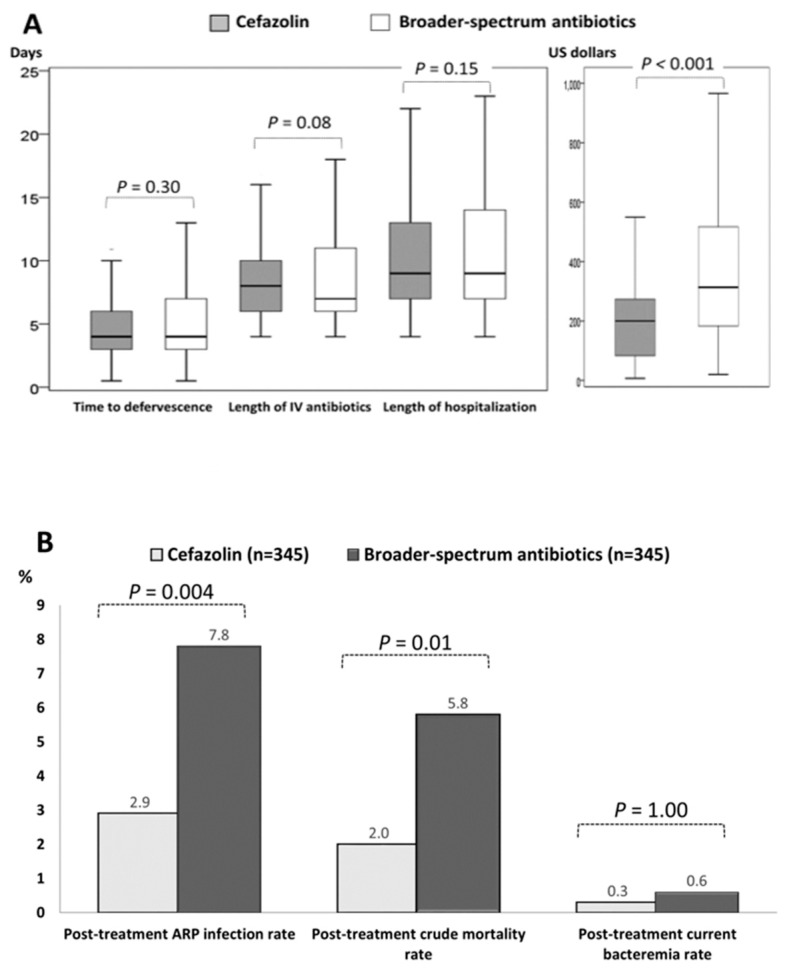
Cefazolin is traditionally active against Escherichia coli, Klebsiella species, and Proteus mirabilis (EKP) isolates. The Clinical and Laboratory Standards Institute (CLSI) has twice updated cefazolin susceptibility breakpoints for EKP since 2010, but its role in the definitive treatment of cefazolin-susceptible EKP bacteremia remains debated. To assess its efficacy as a definitive agent, the 8-year cohort study consisted of 941 adults with monomicrobial cefazolin-susceptible EKP bacteremia, based on the CLSI criteria issued in 2019, was retrospectively established in a medical center. Based on the definitive antimicrobial prescription, eligible patients were categorized into the cefazolin (399 patients, 42.4%) and broader-spectrum antibiotic (BSA) (542, 57.6%) groups. Initially, fewer proportions of patients with fatal comorbidities (the McCabe classification) and the critical illness (a Pitt bacteremia score ≥4) at the onset and day 3 of the bacteremia episode were found in the cefazolin group, compared to the BSA group. After propensity-score matching, no significant difference of patient proportions between the cefazolin (345 patients) and BSA (345) groups was observed, in terms of the elderly, types and severity of comorbidities, bacteremia severity at the onset and day 3, major bacteremia sources, and the 15-day and 30-day crude mortality. In early outcomes, lengths of time to defervescence, intravenous (IV) antimicrobial administration, and hospitalization were similar in the two matched groups; lower costs of IV antimicrobial administration were observed in the cefazolin group. Notably, for late outcomes, lower proportions of post-treatment infections caused by antimicrobial-resistant pathogens (ARPs) and post-treatment mortality rates were evidenced in the cefazolin group. Conclusively, cefazolin is definitively efficacious and cost-effective for adults with community-onset cefazolin-susceptible EKP bacteremia in this one-center study, compared to BSAs. However, a prospective multicenter study should be conducted for external validation with other communities.
头孢唑林传统上对大肠埃希菌、克雷伯菌属和奇异变形杆菌(EKP)分离株具有活性。自2010年以来,临床和实验室标准协会(CLSI)已两次更新EKP的头孢唑林敏感性断点,但其在头孢唑林敏感的EKP菌血症的确定性治疗中的作用仍存在争议。为了评估其作为确定性药物的疗效,在一家医疗中心回顾性建立了一项为期8年的队列研究,该研究纳入了941例符合2019年CLSI标准的单微生物头孢唑林敏感的EKP菌血症成人患者。根据最终的抗菌药物处方,符合条件的患者被分为头孢唑林组(399例患者,42.4%)和广谱抗生素(BSA)组(542例,57.6%)。最初,与BSA组相比,头孢唑林组在菌血症发作时和第3天患有致命合并症(麦凯布分类)和危重病(皮特菌血症评分≥4)的患者比例较低。在倾向评分匹配后,在老年人、合并症的类型和严重程度、发作时和第3天的菌血症严重程度、主要菌血症来源以及15天和30天的粗死亡率方面,未观察到头孢唑林组(345例患者)和BSA组(345例)之间患者比例的显著差异。在早期结果方面,两个匹配组的退热时间、静脉抗菌药物给药时间和住院时间相似;头孢唑林组的静脉抗菌药物给药成本较低。值得注意的是,在晚期结果方面,头孢唑林组中由抗菌药物耐药病原体(ARP)引起的治疗后感染比例和治疗后死亡率较低。总之,在这项单中心研究中,与BSA相比,头孢唑林对于社区获得性头孢唑林敏感的EKP菌血症成人患者具有确切疗效且具有成本效益。然而,应该进行一项前瞻性多中心研究,以便在其他社区进行外部验证。