Department of Obstetrics and Gynecology, Division of Maternal Fetal Medicine, Seoul National University College of Medicine, Seoul, Korea.
Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
PLoS One. 2019 Nov 19;14(11):e0225328. doi: 10.1371/journal.pone.0225328. eCollection 2019.
No information exists about whether fetal inflammatory-response(FIR), early-onset neonatal sepsis(EONS) and chorioamnionitis(an advanced-stage of maternal inflammatory-response in extraplacental membranes) continuously increase according to the progression of inflammation in umbilical-cord(UC). The objective of current-study is to examine this-issue.
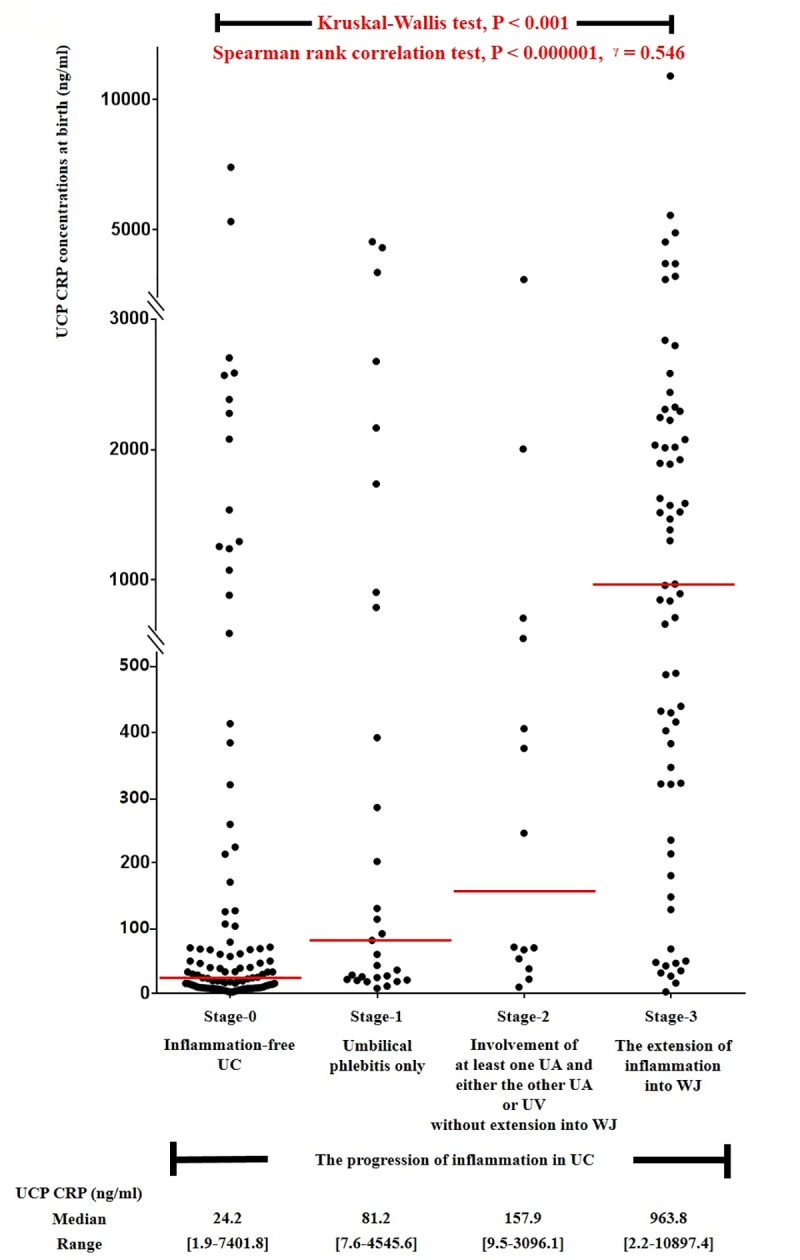
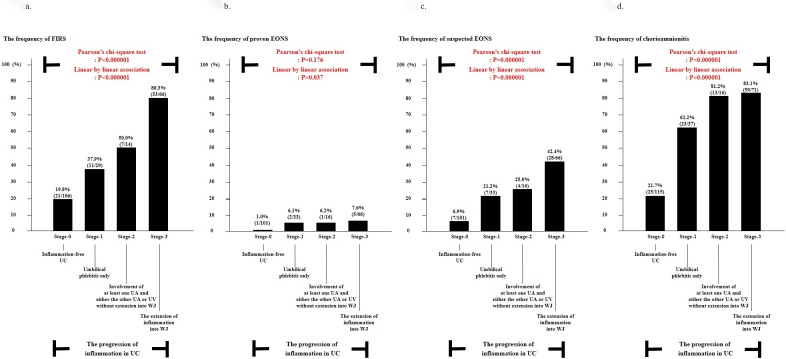
Study-population included 239singleton pregnant-women(gestational-age[GA] at delivery: 21.6~36weeks) who had inflammation in extraplacental membranes or chorionic plate (CP) and either preterm-labor or preterm-PROM. We examined FIR, and the frequency of fetal inflammatory-responses syndrome(FIRS), proven-EONS, suspected-EONS and chorioamnionitis according to the progression of inflammation in UC. The progression of inflammation in UC was divided with a slight-modification from previously reported-criteria as follows: stage0, inflammation-free UC; stage-1: umbilical phlebitis only; stage-2: involvement of at least one UA and either the other UA or UV without extension into WJ; stage-3: the extension of inflammation into WJ. FIR was gauged by umbilical-cord-plasma(UCP) CRP concentration(ng/ml) at birth, and FIRS was defined as an elevated UCP CRP concentration at birth(≥200ng/ml).
Stage-0, stage-1, stage-2 and stage-3 of inflammation in UC were present in 48.1%, 15.5%, 6.7%, and 29.7% of cases. FIR continuously increased according to the progression of inflammation in UC(Kruskal-Wallis test,P<0.001; Spearman-rank-correlation test,P<0.000001,r = 0.546). Moreover, there was a significant and stepwise increase in the frequency of FIRS, proven-EONS, suspected-EONS and chorioamnionitis according to the progression of inflammation in UC(each for P<0.000005 in both chi-square test and linear-by-linear-association). Multiple logistic-regression analysis demonstrated that the more advanced-stage in the progression of inflammation in UC(i.e., stage-1 vs. stage-2 vs. stage-3), the better predictor of suspected-EONS (Odds-ratio[OR]3.358, 95%confidence-interval[CI]:1.020-11.057 vs. OR5.147, 95%CI:1.189-22.275 vs. OR11.040, 95%CI:4.118-29.592) and chorioamnionitis(OR6.593, 95%CI:2.717-15.999 vs. OR16.508, 95%CI:3.916-69.596 vs. OR20.167, 95%CI:8.629-47.137).
FIR, EONS and chorioamnionitis continuously increase according to the progression of inflammation in UC among preterm-gestations with inflammation in extraplacental membranes or CP. This finding may suggest that funisitis(inflammation in UC) is both qualitatively and quantitatively histologic-counterpart of FIRS, and a surrogate-marker for chorioamnionitis.
目前尚无信息表明,胎儿炎症反应(FIR)、早发型新生儿败血症(EONS)和绒毛膜羊膜炎(胎盘外膜炎症的晚期阶段)是否会随着脐带(UC)炎症的进展而持续增加。本研究旨在检验这一问题。
研究人群包括 239 名单胎孕妇(分娩时的孕龄[GA]:21.6~36 周),这些孕妇的胎盘外膜或绒毛板(CP)有炎症,且有早产临产或早产胎膜早破。我们根据 UC 炎症的进展,检查 FIR 以及胎儿炎症反应综合征(FIRS)、确诊 EONS、疑似 EONS 和绒毛膜羊膜炎的发生率。UC 炎症的进展通过对之前报道的标准进行轻微修改来划分,具体如下:阶段 0,UC 无炎症;阶段 1:仅存在脐静脉炎;阶段 2:至少有一条 UA 和另一条 UA 或 UV 受累,但未延伸至 WJ;阶段 3:炎症延伸至 WJ。FIR 通过脐静脉血浆(UCP)CRP 浓度(ng/ml)来评估,出生时 UCP CRP 浓度升高定义为 FIRS(≥200ng/ml)。
UC 炎症的 0 期、1 期、2 期和 3 期分别占 48.1%、15.5%、6.7%和 29.7%。FIR 随着 UC 炎症的进展而持续增加(Kruskal-Wallis 检验,P<0.001;Spearman 秩相关检验,P<0.000001,r=0.546)。此外,随着 UC 炎症的进展,FIRS、确诊 EONS、疑似 EONS 和绒毛膜羊膜炎的发生率呈显著且逐步增加(卡方检验和线性关联检验均 P<0.000005)。多因素逻辑回归分析表明,UC 炎症进展越严重(即阶段 1 比阶段 2 比阶段 3),疑似 EONS 的预测效果越好(优势比[OR]3.358,95%置信区间[CI]:1.020-11.057 比 OR5.147,95%CI:1.189-22.275 比 OR11.040,95%CI:4.118-29.592)和绒毛膜羊膜炎(OR6.593,95%CI:2.717-15.999 比 OR16.508,95%CI:3.916-69.596 比 OR20.167,95%CI:8.629-47.137)。
在胎盘外膜或 CP 有炎症的早产孕妇中,FIR、EONS 和绒毛膜羊膜炎随着 UC 炎症的进展而持续增加。这一发现可能表明,脐带炎(UC 炎症)在组织学上既是 FIRS 的定性和定量表现,也是绒毛膜羊膜炎的替代标志物。