Wong Yin Ping, Khong T Yee
Department of Pathology, Faculty of Medicine, Universiti Kebangsaan Malaysia, Kuala Lumpur 56000, Malaysia.
Department of Pathology, SA Pathology, Women's and Children's Hospital, North Adelaide, SA 5006, Australia.
Diagnostics (Basel). 2023 Jan 29;13(3):487. doi: 10.3390/diagnostics13030487.
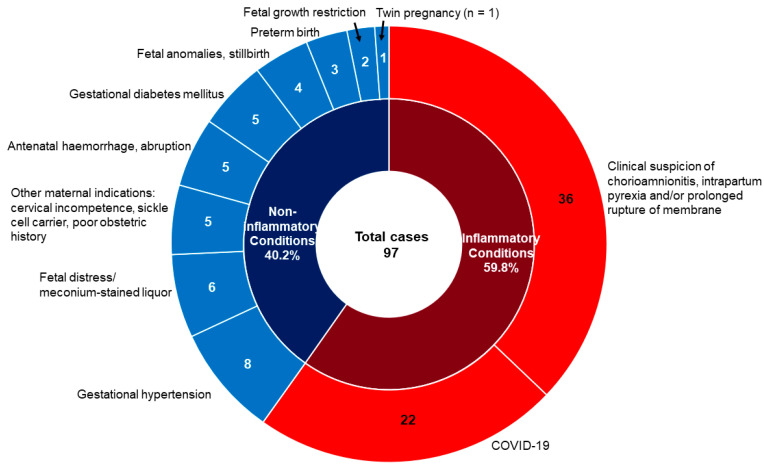
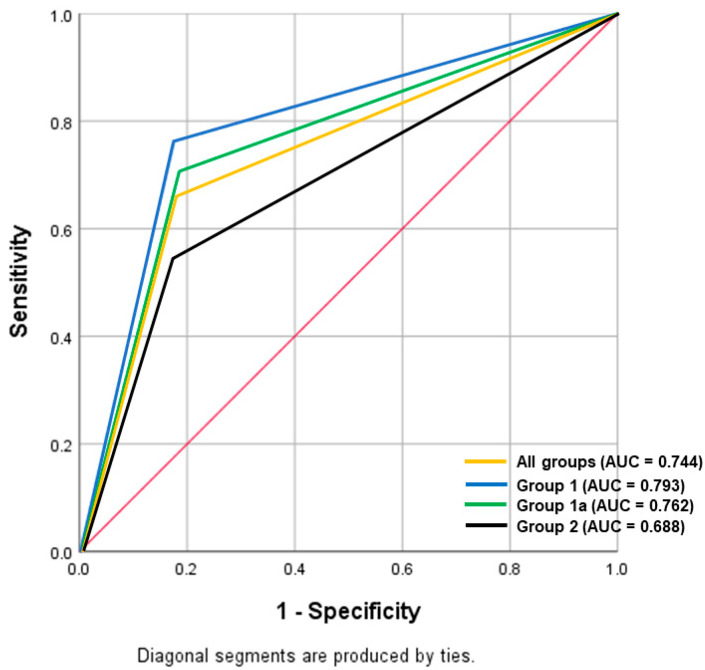
Neonates born with the fetal inflammatory response (FIR) are at risk of complications such as early-onset neonatal sepsis, meningitis, and pneumonia. Providing an early histopathological diagnosis of FIR is important to guide management but can be a challenge in busy laboratories. This is a retrospective cross-sectional study over a four-month duration recruiting all placental cases with histological chorioamnionitis in our institution. The diagnostic performance of the umbilical cord (UC) section in identifying FIR, relative to the corresponding subsequent placental sections, was assessed. Clinical predictors of umbilical cord FIR were also investigated. A total of 390 UC sections were analyzed, of which 206 (52.8%) were found positive for FIR: 111 cases (53.9%) stage 1, 87 (42.2%) stage 2, and 8 (3.9%) stage 3. Our data revealed a good diagnostic sensitivity, specificity, positive predictive value, and accuracy of 76.2% (95%CI: 68.6-82.7%), 82.4% (95%CI: 65.5-93.2%), 95.0% (95%CI: 90.2-97.6%), and 77.3% (95%CI: 70.6-83.1%) respectively, in cases when clinical chorioamnionitis, fever and/or prolonged rupture of membrane (PROM) were suspected, with the area under the curve of 0.793. A maternal inflammatory response (MIR) was correlated with FIR ( < 0.001). Multivariate logistic regression analysis indicated that the higher the gestational age, clinical suspicion of chorioamnionitis, fever, and/or PROM, and the higher the stage of MIR significantly increased the odds of FIR ( < 0.001). UC section diagnosis of FIR is reasonably accurate in cases with clinical chorioamnionitis, fever, and/or PROM. Changing current laboratory practice to rapid processing of UC ahead of the rest of the other placental sections can be recommended in busy pathology departments.
患有胎儿炎症反应(FIR)的新生儿有发生早发性新生儿败血症、脑膜炎和肺炎等并发症的风险。对FIR进行早期组织病理学诊断对于指导治疗很重要,但在繁忙的实验室中可能具有挑战性。这是一项为期四个月的回顾性横断面研究,纳入了我们机构中所有组织学诊断为绒毛膜羊膜炎的胎盘病例。评估了脐带(UC)切片相对于相应后续胎盘切片在识别FIR方面的诊断性能。还研究了脐带FIR的临床预测因素。共分析了390个UC切片,其中206个(52.8%)被发现FIR呈阳性:111例(53.9%)为1期,87例(42.2%)为2期,8例(3.9%)为3期。我们的数据显示,在怀疑有临床绒毛膜羊膜炎、发热和/或胎膜早破(PROM)的病例中,诊断敏感性、特异性、阳性预测值和准确性分别为76.2%(95%CI:68.6 - 82.7%)、82.4%(95%CI:65.5 - 93.2%)、95.0%(95%CI:90.2 - 97.6%)和77.3%(95%CI:70.6 - 83.1%),曲线下面积为0.793。母体炎症反应(MIR)与FIR相关(<0.001)。多因素逻辑回归分析表明,孕周越高、临床怀疑绒毛膜羊膜炎、发热和/或PROM以及MIR分期越高,FIR的发生几率显著增加(<0.001)。在有临床绒毛膜羊膜炎、发热和/或PROM的病例中,UC切片对FIR的诊断相当准确。在繁忙的病理科,建议改变当前的实验室操作流程,在处理其他胎盘切片之前先对UC进行快速处理。