Petri Michelle A, Barr Erik, Magder Laurence S
Rheumatology, Johns Hopkins Medicine, Baltimore, Maryland, USA.
Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland, USA.
Lupus Sci Med. 2019 Oct 10;6(1):e000346. doi: 10.1136/lupus-2019-000346. eCollection 2019.
Accelerated atherosclerosis remains the major cause of late death (after 5 years) in SLE. Yet, the 'traditional' cardiovascular risk equations (such as Framingham) consistently underestimate the risk. We sought to construct a data-driven formula for cardiovascular risk in SLE, based on data collected during the first year in a longitudinal cohort, for research purposes.
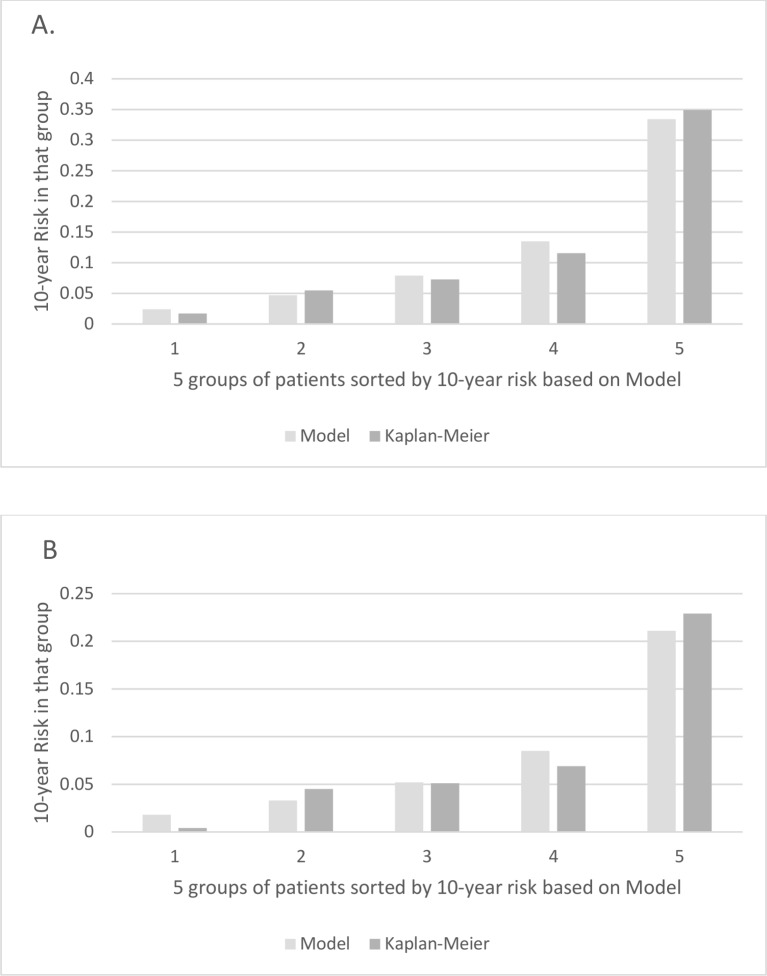
Two risk formulas were derived: one was for a broad set of cardiovascular outcomes (myocardial infarction, stroke, onset of angina, coronary procedures such as bypass or stent, claudication, peripheral artery disease or congestive heart failure); and the other for hard outcomes (myocardial infarction or stroke). Traditional and SLE-specific risk factors for cardiovascular disease were measured during the first year of cohort participation. Using Cox proportional hazards modelling, SLE formulas to calculate the 10-year risk of a subsequent cardiovascular event were derived and compared with the Framingham (for the broader outcome) and American College of Cardiology formulas (for the hard outcomes).
SLE-related risk factors for each model included mean disease activity score (as measured by the SELENA revision of the SLE Disease Activity Index), low C3 and history of lupus anticoagulant. In those with SLE-related risk factors, the estimated 10-year risk based on our formula was substantially higher than the risk estimated based on the formulas for the general population.
The excess cardiovascular risk among patients with SLE varies substantially depending on the SLE-related risk factors, age and traditional risk factors. Cardiovascular risk formulas based on individual data from patients with SLE may better estimate 10-year cardiovascular risk among patients with SLE than the Framingham or American College of Cardiology equations.
加速动脉粥样硬化仍是系统性红斑狼疮(SLE)患者5年后晚期死亡的主要原因。然而,“传统”的心血管风险评估公式(如弗雷明汉姆公式)一直低估了该风险。我们旨在基于纵向队列研究第一年收集的数据,构建一个数据驱动的SLE心血管风险公式,用于研究目的。
推导了两个风险公式:一个用于广泛的心血管结局(心肌梗死、中风、心绞痛发作、冠状动脉搭桥或支架置入等介入治疗、间歇性跛行、外周动脉疾病或充血性心力衰竭);另一个用于严重结局(心肌梗死或中风)。在队列研究参与的第一年测量传统和SLE特异性心血管疾病风险因素。使用Cox比例风险模型,推导了计算后续心血管事件10年风险的SLE公式,并与弗雷明汉姆公式(用于更广泛的结局)和美国心脏病学会公式(用于严重结局)进行比较。
每个模型中与SLE相关的风险因素包括平均疾病活动评分(通过SLE疾病活动指数的SELENA修订版测量)、低C3水平和狼疮抗凝物病史。在具有SLE相关风险因素的患者中,基于我们公式估计的10年风险显著高于基于一般人群公式估计的风险。
SLE患者中额外的心血管风险因SLE相关风险因素、年龄和传统风险因素的不同而有很大差异。基于SLE患者个体数据的心血管风险公式可能比弗雷明汉姆公式或美国心脏病学会公式能更好地估计SLE患者的10年心血管风险。