Heestermans Tessa, Payne Beth, Kayode Gbenga Ayodele, Amoakoh-Coleman Mary, Schuit Ewoud, Rijken Marcus J, Klipstein-Grobusch Kerstin, Bloemenkamp Kitty, Grobbee Diederick E, Browne Joyce L
Julius Global Health, Julius Center for Health Sciences and Primary Care, Universitair Medisch Centrum Utrecht, Utrecht University, Utrecht, The Netherlands.
Women's Health Research Institute, School of Population and Public Health, The University of British Columbia, Vancouver, British Columbia, Canada.
BMJ Glob Health. 2019 Oct 30;4(5):e001759. doi: 10.1136/bmjgh-2019-001759. eCollection 2019.
Ninety-nine per cent of all maternal and neonatal deaths occur in low-income and middle-income countries (LMIC). Prognostic models can provide standardised risk assessment to guide clinical management and can be vital to reduce and prevent maternal and perinatal mortality and morbidity. This review provides a comprehensive summary of prognostic models for adverse maternal and perinatal outcomes developed and/or validated in LMIC.
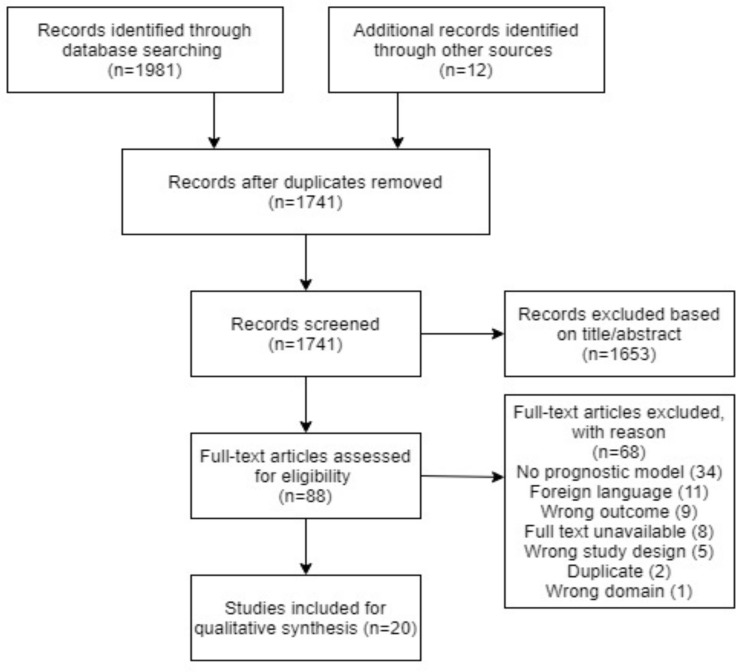
A systematic search in four databases (PubMed/Medline, EMBASE, Global Health Library and The Cochrane Library) was conducted from inception (1970) up to 2 May 2018. Risk of bias was assessed with the PROBAST tool and narratively summarised.
1741 articles were screened and 21 prognostic models identified. Seventeen models focused on maternal outcomes and four on perinatal outcomes, of which hypertensive disorders of pregnancy (n=9) and perinatal death including stillbirth (n=4) was most reported. Only one model was externally validated. Thirty different predictors were used to develop the models. Risk of bias varied across studies, with the item 'quality of analysis' performing the least.
Prognostic models can be easy to use, informative and low cost with great potential to improve maternal and neonatal health in LMIC settings. However, the number of prognostic models developed or validated in LMIC settings is low and mirrors the 10/90 gap in which only 10% of resources are dedicated to 90% of the global disease burden. External validation of existing models developed in both LMIC and high-income countries instead of developing new models should be encouraged.
CRD42017058044.
99%的孕产妇和新生儿死亡发生在低收入和中等收入国家(LMIC)。预后模型可以提供标准化的风险评估以指导临床管理,对于降低和预防孕产妇及围产期死亡率和发病率至关重要。本综述全面总结了在低收入和中等收入国家开发和/或验证的不良孕产妇和围产期结局的预后模型。
对四个数据库(PubMed/Medline、EMBASE、全球健康图书馆和考克兰图书馆)进行了从起始时间(1970年)至2018年5月2日的系统检索。使用PROBAST工具评估偏倚风险并进行叙述性总结。
筛选了1741篇文章,确定了21个预后模型。17个模型关注孕产妇结局,4个关注围产期结局,其中妊娠高血压疾病(n = 9)和包括死产在内的围产期死亡(n = 4)报道最多。只有一个模型进行了外部验证。使用了30种不同的预测因素来开发这些模型。不同研究的偏倚风险各不相同,其中“分析质量”这一项表现最差。
预后模型易于使用、信息丰富且成本低廉,在改善低收入和中等收入国家孕产妇和新生儿健康方面具有巨大潜力。然而,在低收入和中等收入国家开发或验证的预后模型数量较少,反映了10/90差距,即仅10%的资源用于应对90%的全球疾病负担。应鼓励对在低收入和中等收入国家以及高收入国家开发的现有模型进行外部验证,而非开发新模型。
PROSPERO注册号:CRD42017058044。