Université de Paris, Epidemiology and Statistics Research Center/CRESS, INSERM, INRA, F-75004, Paris, France.
Elizabeth Garrett Anderson Institute for Womens' Health, UCL, London, UK.
BMC Pediatr. 2019 Nov 21;19(1):451. doi: 10.1186/s12887-019-1827-6.
Gaining a better understanding of the probability, timing and prediction of rehospitalisation amongst preterm babies could help improve outcomes. There is limited research addressing these topics amongst extremely and very preterm babies. In this context, unplanned rehospitalisations constitute an important, potentially modifiable adverse event. We aimed to establish the probability, time-distribution and predictability of unplanned rehospitalisation within 30 days of discharge in a population of French preterm babies.
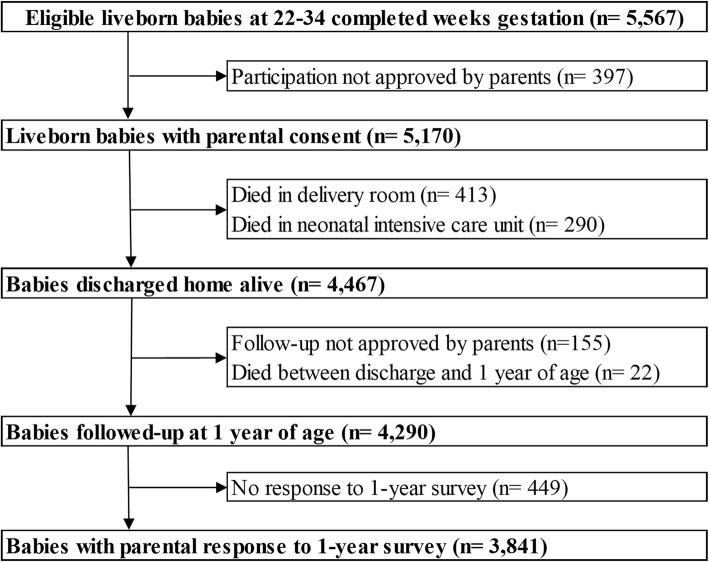
This study used data from EPIPAGE 2, a population-based prospective study of French preterm babies. Only those babies discharged home alive and whose parents responded to the one-year survey were eligible for inclusion in our study. For Kaplan-Meier analysis, the outcome was unplanned rehospitalisation censored at 30 days. For predictive modelling, the outcome was binary, recording unplanned rehospitalisation within 30 days of discharge. Predictors included routine clinical variables selected based on expert opinion.
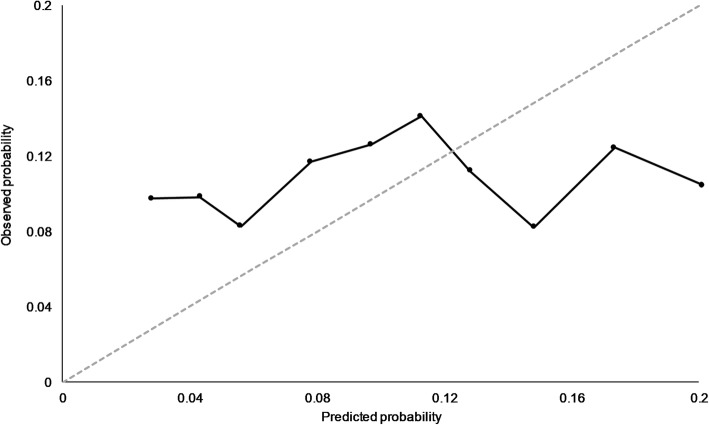
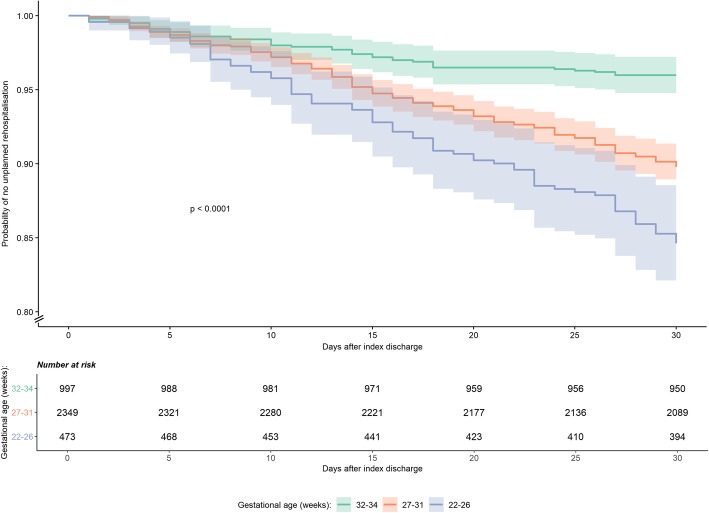
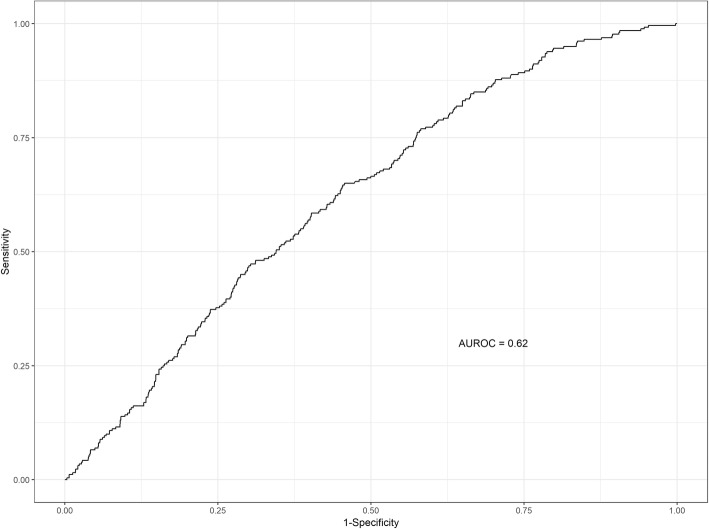
Of 3841 eligible babies, 350 (9.1, 95% CI 8.2-10.1) experienced an unplanned rehospitalisation within 30 days. The probability of rehospitalisation progressed at a consistent rate over the 30 days. There were significant differences in rehospitalisation probability by gestational age. The cross-validated performance of a ten predictor model demonstrated low discrimination and calibration. The area under the receiver operating characteristic curve was 0.62 (95% CI 0.59-0.65).
Unplanned rehospitalisation within 30 days of discharge was infrequent and the probability of rehospitalisation progressed at a consistent rate. Lower gestational age increased the probability of rehospitalisation. Predictive models comprised of clinically important variables had limited predictive ability.
更好地了解早产儿再次住院的概率、时间和预测因素,可能有助于改善预后。在极早产儿和超低出生体重儿中,针对这些问题的研究有限。在这种情况下,计划外再次住院是一个重要的、潜在可改变的不良事件。我们旨在确定法国早产儿出院后 30 天内计划外再次住院的概率、时间分布和可预测性。
本研究使用了 EPIPAGE 2 的数据,这是一项针对法国早产儿的基于人群的前瞻性研究。只有那些活着出院且父母回应了一年期调查的婴儿才有资格纳入本研究。对于 Kaplan-Meier 分析,结局是 30 天内计划外再次住院的情况。对于预测模型,结局是二分类的,记录出院后 30 天内计划外再次住院的情况。预测因素包括根据专家意见选择的常规临床变量。
在 3841 名符合条件的婴儿中,350 名(9.1%,95%CI 8.2-10.1)在 30 天内出现了计划外再次住院。再入院的概率在 30 天内以稳定的速度增加。再入院的概率因胎龄而异。十个预测因素模型的交叉验证表现出低的区分度和校准度。受试者工作特征曲线下面积为 0.62(95%CI 0.59-0.65)。
出院后 30 天内计划外再次住院的情况并不常见,再入院的概率以稳定的速度增加。胎龄较低会增加再次住院的概率。由临床重要变量组成的预测模型预测能力有限。