Center for Outcomes Research and Evaluation, Yale-New Haven Hospital, New Haven, Conn.
Division of Cardiology, University of Texas Southwestern Medical Center, Dallas, Tex.
Am J Med. 2018 Nov;131(11):1324-1331.e14. doi: 10.1016/j.amjmed.2018.06.013. Epub 2018 Sep 7.
Temporal changes in the readmission rates for patient groups and conditions that were not directly under the purview of the Hospital Readmissions Reduction Program (HRRP) can help assess whether efforts to lower readmissions extended beyond targeted patients and conditions.
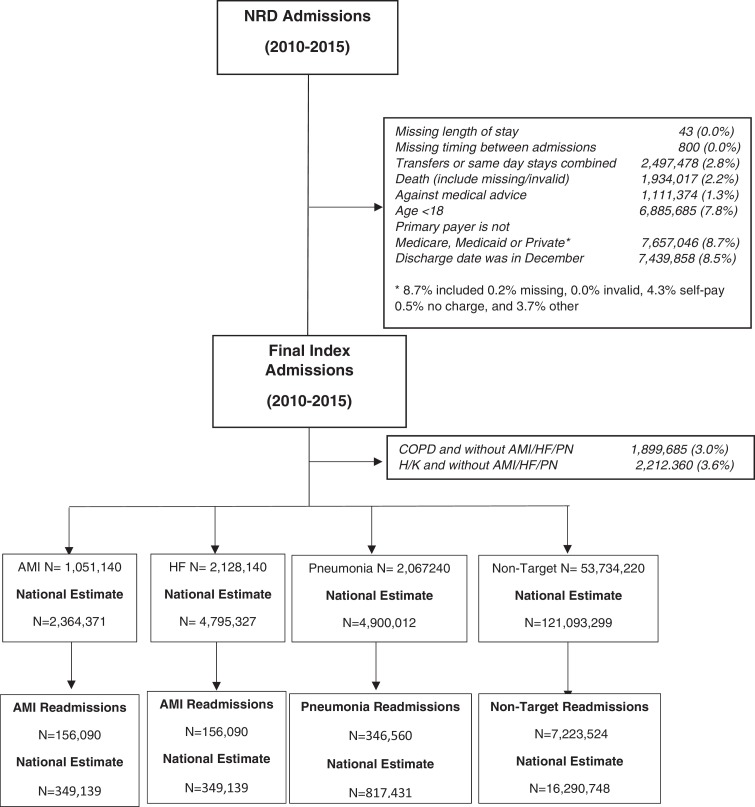
Using the Nationwide Readmissions Database (2010-2015), we assessed trends in all-cause readmission rates for 1 of the 3 HRRP conditions (acute myocardial infarction, heart failure, pneumonia) or conditions not targeted by the HRRP in age-insurance groups defined by age group (≥65 years or <65 years) and payer (Medicare, Medicaid, or private insurance).
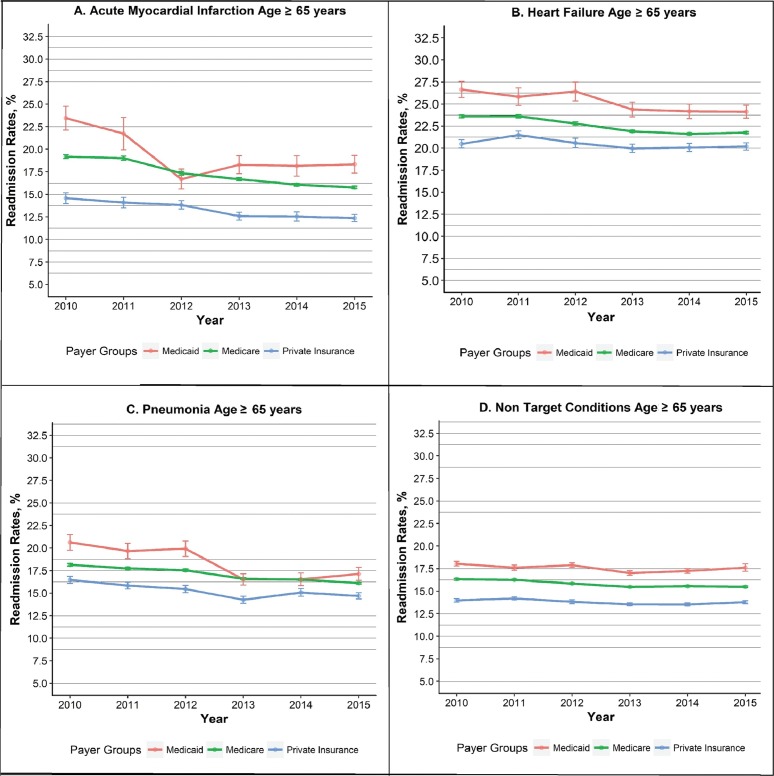
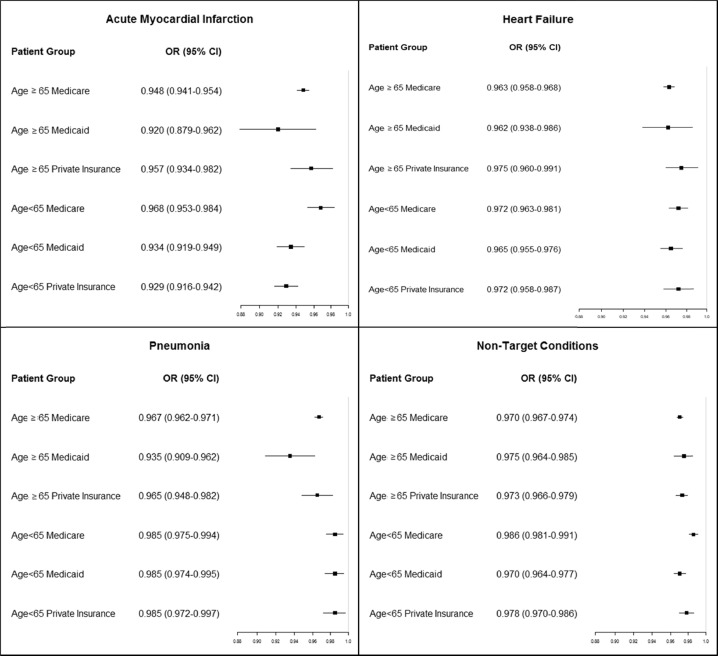
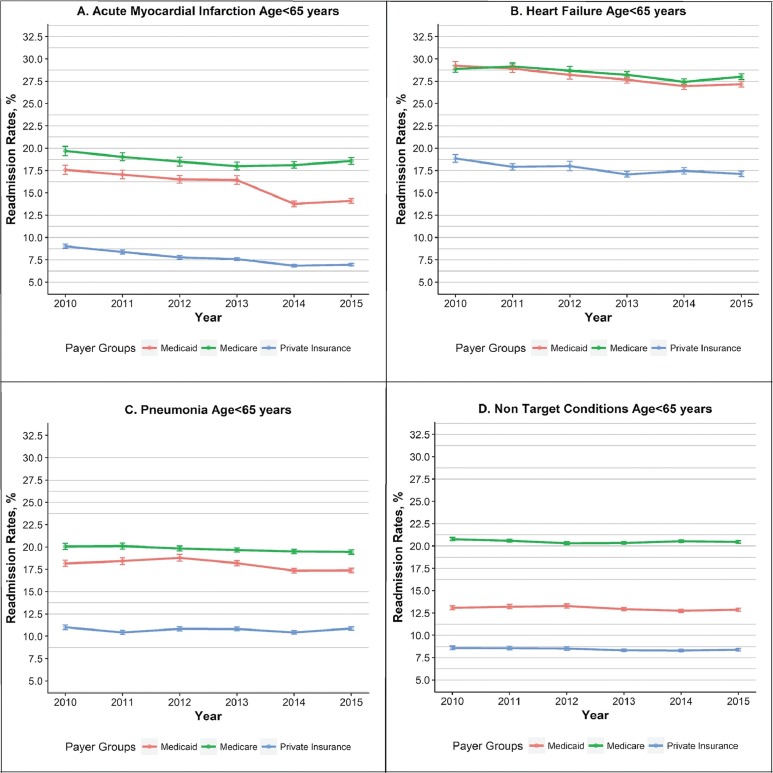
In the group aged ≥65 years, readmission rates for those covered by Medicare, Medicaid, and private insurance decreased annually for acute myocardial infarction (risk-adjusted odds ratio [OR; 95% confidence interval] among Medicare patients, 0.94 [0.94-0.95], among Medicaid patients, 0.93 [0.90-0.97], and among patients with private-insurance, 0.95 [0.93-0.97]); heart failure (ORs, 0.96 [0.96-0.97], 0.96 [0.94-0.98], and 0.97 [0.96-0.99], for the 3 payers, respectively), and pneumonia (ORs, 0.96 [0.96-0.97), 0.94 [0.92-0.96], and 0.96 [0.95-0.97], respectively). Readmission rates also decreased in the group aged <65 years for acute myocardial infarction (ORs: Medicare 0.97 [0.96-0.98], Medicaid 0.94 [0.92-0.95], and private insurance 0.93 [0.92-0.94]), heart failure (ORs, 0.98 [0.97-0.98]: 0.96 [0.96-0.97], and 0.97 [0.95-0.98], for the 3 payers, respectively), and pneumonia (ORs, 0.98 [0.97-0.99], 0.98 [0.97-0.99], and 0.98 [0.97-1.00], respectively). Further, readmission rates decreased significantly for non-target conditions.
There appears to be a systematic improvement in readmission rates for patient groups beyond the population of fee-for-service, older, Medicare beneficiaries included in the HRRP.
评估医院再入院率降低计划(HRRP)未直接涉及的患者群体和病症的再入院率的时间变化,有助于评估降低再入院率的努力是否超出了目标患者和病症。
利用全国再入院数据库(2010-2015 年),我们评估了 3 个 HRRP 病症(急性心肌梗死、心力衰竭、肺炎)或 HRRP 未涉及的病症在按年龄(≥65 岁或<65 岁)和保险类型(医疗保险、医疗补助或私人保险)定义的年龄保险组中的全因再入院率的趋势。
在≥65 岁的年龄组中,医疗保险、医疗补助和私人保险覆盖的患者的急性心肌梗死再入院率逐年下降(医疗保险患者的风险调整后比值比[OR;95%置信区间]为 0.94[0.94-0.95],医疗补助患者为 0.93[0.90-0.97],私人保险患者为 0.95[0.93-0.97]);心力衰竭(ORs,0.96[0.96-0.97],0.96[0.94-0.98]和 0.97[0.96-0.99],分别为 3 种支付方式)和肺炎(ORs,0.96[0.96-0.97],0.94[0.92-0.96]和 0.96[0.95-0.97],分别为 3 种支付方式)。在<65 岁的年龄组中,急性心肌梗死(ORs:医疗保险 0.97[0.96-0.98],医疗补助 0.94[0.92-0.95],私人保险 0.93[0.92-0.94])、心力衰竭(ORs,0.98[0.97-0.98]:0.96[0.96-0.97]和 0.97[0.95-0.98],分别为 3 种支付方式)和肺炎(ORs,0.98[0.97-0.99],0.98[0.97-0.99]和 0.98[0.97-1.00],分别为 3 种支付方式)的再入院率也有所下降。此外,非目标病症的再入院率显著下降。
除了 HRRP 中包含的按服务收费、年龄较大、医疗保险受益人的人群外,似乎有系统地改善了患者群体的再入院率。