Gaborit Benjamin Jean, Tessoulin Benoit, Lavergne Rose-Anne, Morio Florent, Sagan Christine, Canet Emmanuel, Lecomte Raphael, Leturnier Paul, Deschanvres Colin, Khatchatourian Lydie, Asseray Nathalie, Garret Charlotte, Vourch Michael, Marest Delphine, Raffi François, Boutoille David, Reignier Jean
Department of Infectious Diseases, Hôtel-Dieu University Hospital, University Hospital of Nantes and CIC 1413, INSERM, 1 Place Alexis-Ricordeau, 44000, Nantes, France.
EA 3826, Laboratory of Clinical and Experimental Therapeutics of Infections, IRS2-Nantes Biotech, Nantes, France.
Ann Intensive Care. 2019 Nov 27;9(1):131. doi: 10.1186/s13613-019-0604-x.
Pneumocystis jirovecii pneumonia (PJP) remains a severe disease associated with high rates of invasive mechanical ventilation (MV) and mortality. The objectives of this study were to assess early risk factors for severe PJP and 90-day mortality, including the broncho-alveolar lavage fluid cytology profiles at diagnosis.
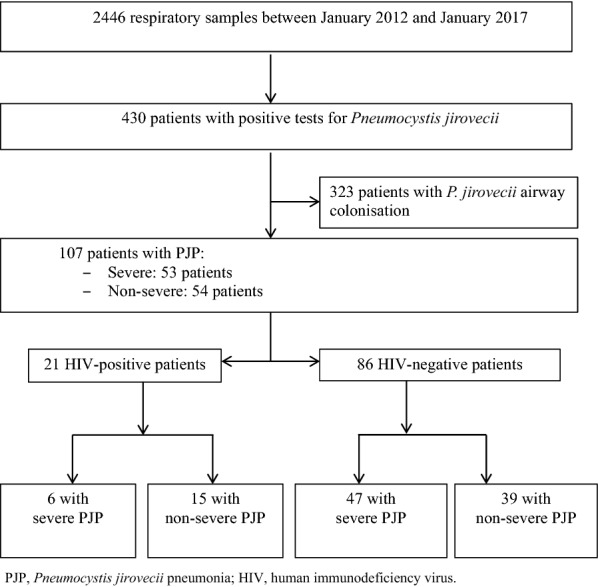
We prospectively enrolled all patients meeting pre-defined diagnostic criteria for PJP admitted at Nantes university hospital, France, from January 2012 to January 2017. Diagnostic criteria for PJP were typical clinical features with microbiological confirmation of P. jirovecii cysts by direct examination or a positive specific quantitative real-time polymerase chain reaction (PCR) assay. Severe PJP was defined as hypoxemic acute respiratory failure requiring high-flow nasal oxygen with at least 50% FiO, non-invasive ventilation, or MV.
Of 2446 respiratory samples investigated during the study period, 514 from 430 patients were positive for P. jirovecii. Of these 430 patients, 107 met criteria for PJP and were included in the study, 53 (49.5%) patients had severe PJP, including 30 who required MV. All patients were immunocompromised with haematological malignancy ranking first (n = 37, 35%), followed by solid organ transplantation (n = 27, 25%), HIV-infection (n = 21, 20%), systemic diseases (n = 13, 12%), solid tumors (n = 12, 11%) and primary immunodeficiency (n = 6, 8%). By multivariate analysis, factors independently associated with severity were older age (OR, 3.36; 95% CI 1.4-8.5; p < 0.05), a P. jirovecii microscopy-positive result from bronchoalveolar lavage (BAL) (OR, 1.3; 95% CI 1.54-9.3; p < 0.05); and absence of a BAL fluid alveolitis profile (OR, 3.2; 95% CI 1.27-8.8; p < 0.04). The 90-day mortality rate was 27%, increasing to 50% in the severe PJP group. Factors independently associated with 90-day mortality were worse SOFA score on day 1 (OR, 1.05; 95% CI 1.02-1.09; p < 0.001) whereas alveolitis at BAL was protective (OR, 0.79; 95% CI 0.65-0.96; p < 0.05). In the subgroup of HIV-negative patients, similar findings were obtained, then viral co-infection were independently associated with higher 90-day mortality (OR, 1.25; 95% CI 1.02-1.55; p < 0.05).
Older age and P. jirovecii oocysts at microscopic examination of BAL were independently associated with severe PJP. Both initial PJP severity as evaluated by the SOFA score and viral co-infection predicted 90-day mortality. Alveolitis at BAL examination was associated with less severe PJP. The pathophysiological mechanism underlying this observation deserves further investigation.
耶氏肺孢子菌肺炎(PJP)仍然是一种严重疾病,与高侵袭性机械通气(MV)率和死亡率相关。本研究的目的是评估重症PJP和90天死亡率的早期危险因素,包括诊断时支气管肺泡灌洗(BAL)液的细胞学特征。
我们前瞻性纳入了2012年1月至2017年1月在法国南特大学医院收治的所有符合PJP预定义诊断标准的患者。PJP的诊断标准为具有典型临床特征,通过直接检查或阳性特异性定量实时聚合酶链反应(PCR)检测微生物学确认耶氏肺孢子菌囊肿。重症PJP定义为低氧性急性呼吸衰竭,需要至少50% FiO₂的高流量鼻导管吸氧、无创通气或MV。
在研究期间调查的2446份呼吸道样本中,来自430例患者的514份样本耶氏肺孢子菌呈阳性。在这430例患者中,107例符合PJP标准并纳入研究,53例(49.5%)患者患有重症PJP,其中30例需要MV。所有患者均免疫功能低下,血液系统恶性肿瘤位居首位(n = 37,35%),其次是实体器官移植(n = 27,25%)、HIV感染(n = 21,20%)、全身性疾病(n = 13,12%)、实体瘤(n = 12,11%)和原发性免疫缺陷(n = 6,8%)。通过多变量分析,与病情严重程度独立相关的因素为年龄较大(OR,3.36;95% CI 1.4 - 8.5;p < 0.05)、BAL的耶氏肺孢子菌显微镜检查阳性结果(OR,1.3;95% CI 1.54 - 9.3;p < 0.05);以及BAL液无肺泡炎特征(OR,3.2;95% CI 1.27 - 8.8;p < 0.04)。90天死亡率为27%,在重症PJP组中升至50%。与90天死亡率独立相关的因素为第1天SOFA评分更差(OR,1.05;95% CI 1.02 - 1.09;p < 0.001),而BAL时的肺泡炎具有保护作用(OR,0.79;95% CI 0.65 - 0.96;p < 0.05)。在HIV阴性患者亚组中,获得了类似的结果,然后病毒合并感染与更高的90天死亡率独立相关(OR,1.25;95% CI 1.02 - 1.55;p < 0.05)。
年龄较大和BAL显微镜检查发现耶氏肺孢子菌卵囊与重症PJP独立相关。通过SOFA评分评估的初始PJP严重程度和病毒合并感染均预测90天死亡率。BAL检查时的肺泡炎与病情较轻的PJP相关。这一观察结果背后的病理生理机制值得进一步研究。