Panetta Carmelo J, Galbraith Erin M, Yanavitski Marat, Koller Patrick K, Shah Binita, Iqbal Sohah, Cigarroa Joaquin E, Gordon Gregory, Rao Sunil V
UMP Heart Care, St. Joseph Hospital, St. Paul, Minnesota.
Heart Care East, University of Minnesota, Minneapolis, Minnesota.
Catheter Cardiovasc Interv. 2020 Jan;95(1):7-12. doi: 10.1002/ccd.28629. Epub 2019 Dec 3.
Investigation of novel vertical radiation shield (VRS) in reducing operator radiation exposure.
Radiation exposure to the operator remains an occupational health hazard in the cardiac catheterization laboratory (CCL).
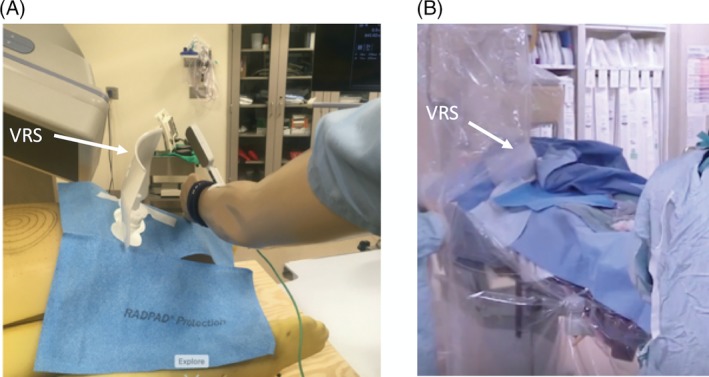
A mannequin simulating an operator was placed near a computational phantom, simulating a patient. Measurement of dose equivalent and Air Kerma located the angle with the highest radiation, followed by a common magnification (8 in.) and comparison of horizontal radiation absorbing pads (HRAP) with or without VRS with two different: CCL, phantoms, and dosimeters. Physician exposure was subsequently measured prospectively with or without VRS during clinical procedures.
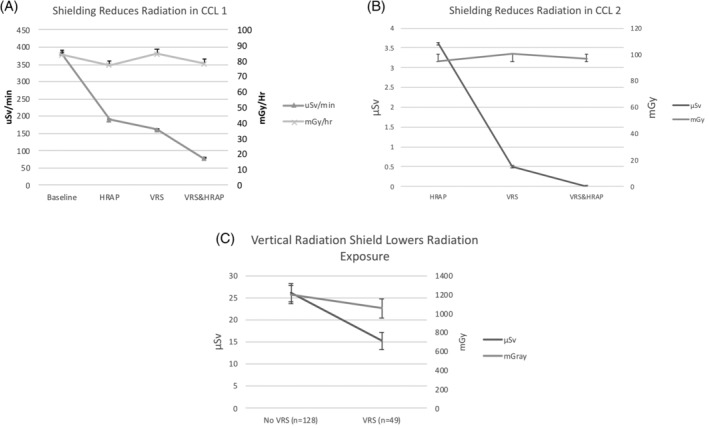
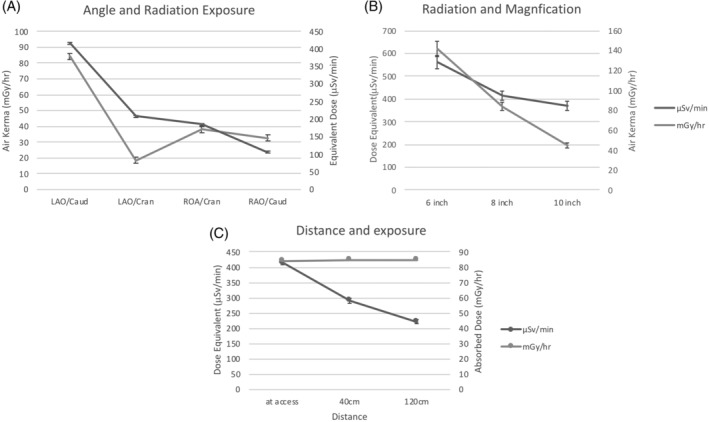
Dose equivalent and Air Kerma to the mannequin was highest at left anterior oblique (LAO)-caudal angle (p < .005). Eight-inch magnification increased mGray by 86.5% and μSv/min by 12.2% compared to 10-in. (p < .005). Moving 40 cm from the access site lowered μSv/min by 30% (p < .005). With LAO-caudal angle and 8-in. magnification, VRS reduced μSv/min by 59%, (p < .005) in one CCL and μSv by 100% (p = .016) in second CCL in addition to HRAP. Prospective study of 177 procedures with HRAP, found VRS lowered μSv by 41.9% (μSv: 15.2 ± 13.4 vs. 26.2 ± 31.4, p = .001) with no difference in mGray. The difference was significant after multivariate adjustment for specified variables (p < .001).
Operator radiation exposure is significantly reduced utilizing a novel VRS, HRAP, and distance from the X-ray tube, and consideration of lower magnification and avoiding LAO-caudal angles to lower radiation for both operator and patient.
研究新型垂直辐射屏蔽装置(VRS)对减少术者辐射暴露的作用。
在心脏导管实验室(CCL)中,术者受到辐射暴露仍是一种职业健康危害。
将模拟术者的人体模型放置在靠近模拟患者的计算体模附近。测量剂量当量和空气比释动能,确定辐射最高的角度,然后采用常用的放大倍数(8英寸),并比较有或无VRS的水平辐射吸收垫(HRAP)在两种不同的CCL、体模和剂量计中的情况。随后在临床操作过程中对有或无VRS时的术者暴露情况进行前瞻性测量。
人体模型的剂量当量和空气比释动能在左前斜位(LAO)-尾位角度时最高(p < 0.005)。与10英寸相比,8英寸放大倍数使毫戈瑞增加86.5%,每分钟微希沃特增加12.2%(p < 0.005)。从进针部位移开40厘米可使每分钟微希沃特降低30%(p < 0.005)。在LAO-尾位角度和8英寸放大倍数下,在一个CCL中,VRS除了HRAP外,还使每分钟微希沃特降低59%(p < 0.005),在第二个CCL中使微希沃特降低100%(p = 0.016)。对177例使用HRAP的操作进行前瞻性研究发现,VRS使微希沃特降低41.9%(微希沃特:15.2±13.4对26.2±31.4,p = 0.001),毫戈瑞无差异。在对特定变量进行多变量调整后,差异具有统计学意义(p < 0.001)。
使用新型VRS、HRAP以及与X射线管保持一定距离可显著降低术者的辐射暴露,同时考虑采用较低放大倍数并避免LAO-尾位角度,以降低术者和患者所受的辐射。