Muench Lukas N, Kia Cameron, Jerliu Aulon, Murphy Matthew, Berthold Daniel P, Cote Mark P, Arciero Robert A, Mazzocca Augustus D
Department of Orthopedic Surgery, UConn Health, Farmington, Connecticut, USA.
Department of Orthopaedic Sports Medicine, Technical University of Munich, Munich, Germany.
Orthop J Sports Med. 2019 Nov 26;7(11):2325967119884539. doi: 10.1177/2325967119884539. eCollection 2019 Nov.
Acromioclavicular (AC) joint separation is a common injury. The anatomic coracoclavicular ligament reconstruction (ACCR) technique is a viable treatment option, designed to restore the native joint anatomy.
To evaluate the clinical and radiographic outcomes of patients undergoing ACCR for the treatment of type III and V AC joint injuries with a minimum 2-year follow-up.
Case series; Level of evidence, 4.
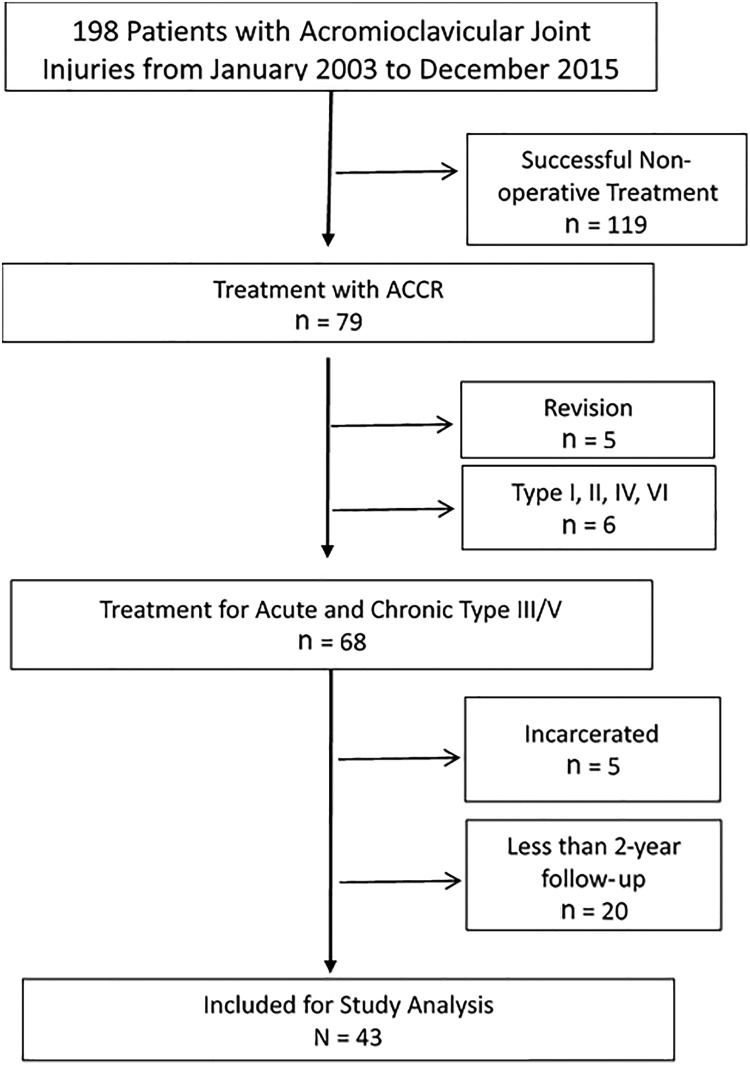
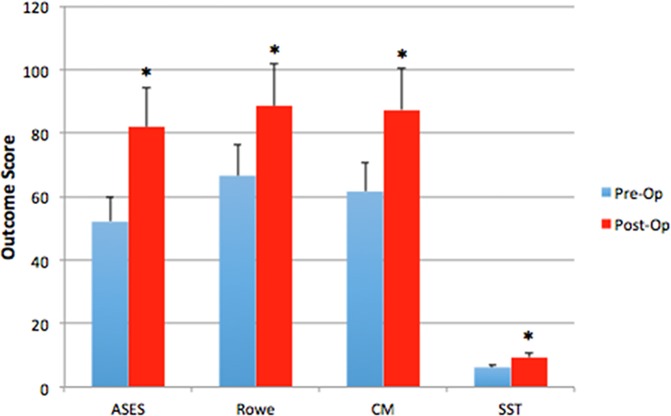
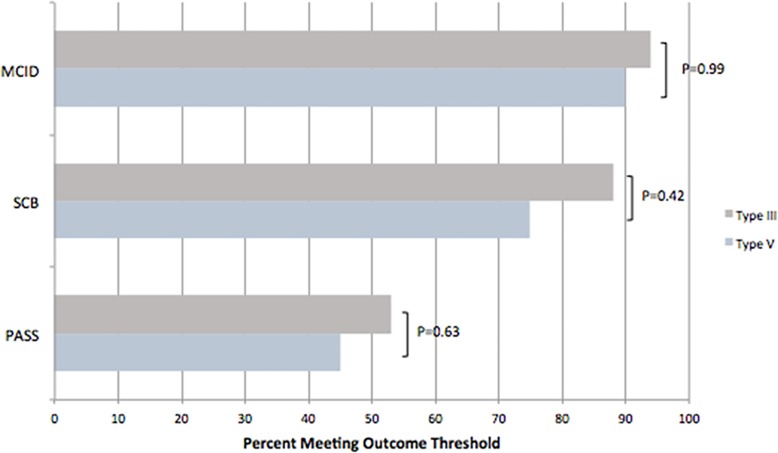
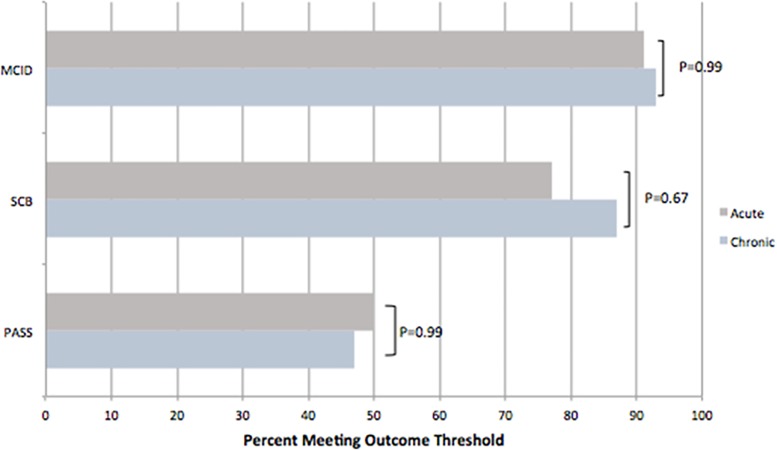
A retrospective chart review was performed on prospectively collected data. Patients who underwent ACCR for type III or V AC joint injuries between January 2003 and December 2015 were analyzed. Clinical outcome measures included the American Shoulder and Elbow Surgeons (ASES) score, Rowe score, Simple Shoulder Test (SST), and Constant-Murley (CM) score. To determine the clinical relevance of the ASES score, the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptomatic state (PASS) were used. The pre- and postoperative coracoclavicular distance (CCD) and side-to-side difference in the CCD were measured for radiographic analysis.
A total of 43 patients (22 acute, 21 chronic) were included in the study. The mean patient age was 43.4 ± 11.4 years, with a mean follow-up of 3.4 years (range, 2.0-7.5 years). With regard to the ASES score, 92% of patients achieved the MCID, 81% achieved the SCB, and 49% reached or exceeded the PASS. There was no significant difference when stratifying by type (III vs V) or chronicity (acute vs chronic) of injury (both > .05). The Rowe score improved from 66.6 ± 15.9 preoperatively to 88.6 ± 12.3 postoperatively, the CM score from 61.6 ± 18.8 to 87.4 ± 15.1, and the SST score from 6.2 ± 3.6 to 9.4 ± 3.7 (all < .001). The postoperative side-to-side difference in the CCD was 3.1 ± 2.7 mm, with type III injuries (2.4 ± 1.9 mm) showing significantly lower measurements compared with type V (4.2 ± 3.4 mm) ( = .02). No significant trend was found between joint reduction and the improvement in clinical outcomes ( > .05).
Patients undergoing ACCR for acute and chronic type III and V AC joint injuries maintained significant improvement in clinical and radiographic outcomes at a minimum 2-year follow-up. Additionally, 81% of patients reached the SCB after surgical reconstruction.
肩锁关节分离是一种常见损伤。解剖学喙锁韧带重建(ACCR)技术是一种可行的治疗选择,旨在恢复关节的自然解剖结构。
评估接受ACCR治疗III型和V型肩锁关节损伤且随访至少2年的患者的临床和影像学结果。
病例系列;证据等级,4级。
对前瞻性收集的数据进行回顾性图表审查。分析2003年1月至2015年12月期间接受ACCR治疗III型或V型肩锁关节损伤的患者。临床结果指标包括美国肩肘外科医师(ASES)评分、Rowe评分、简单肩部测试(SST)和Constant-Murley(CM)评分。为确定ASES评分的临床相关性,使用了最小临床重要差异(MCID)、显著临床获益(SCB)和患者可接受症状状态(PASS)。测量术前和术后的喙锁间距(CCD)以及CCD的左右差异以进行影像学分析。
本研究共纳入43例患者(22例急性,21例慢性)。患者平均年龄为43.4±11.4岁,平均随访3.4年(范围2.0 - 7.5年)。关于ASES评分,92%的患者达到MCID,81%的患者达到SCB,49%的患者达到或超过PASS。按损伤类型(III型与V型)或损伤的慢性程度(急性与慢性)分层时无显著差异(均>0.05)。Rowe评分从术前的66.6±15.9提高到术后的88.6±12.3,CM评分从61.6±18.8提高到87.4±15.1,SST评分从6.2±3.6提高到9.4±3.7(均<0.001)。术后CCD的左右差异为3.1±2.7 mm,III型损伤(2.4±1.9 mm)的测量值显著低于V型损伤(4.2±3.4 mm)(P = 0.02)。未发现关节复位与临床结果改善之间存在显著趋势(P>0.05)。
接受ACCR治疗急性和慢性III型及V型肩锁关节损伤的患者在至少2年的随访中临床和影像学结果保持显著改善。此外,81%的患者在手术重建后达到SCB。