Nephrology Research Unit, Department of Clinical Tropical Medicine, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Immunology Unit, Department of Microbiology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Sci Rep. 2019 Dec 18;9(1):19356. doi: 10.1038/s41598-019-55833-0.
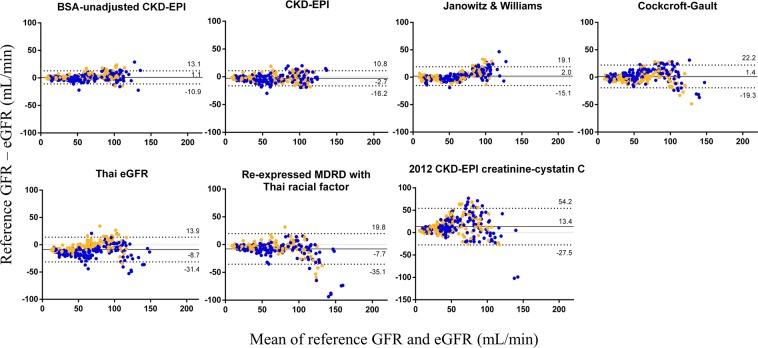
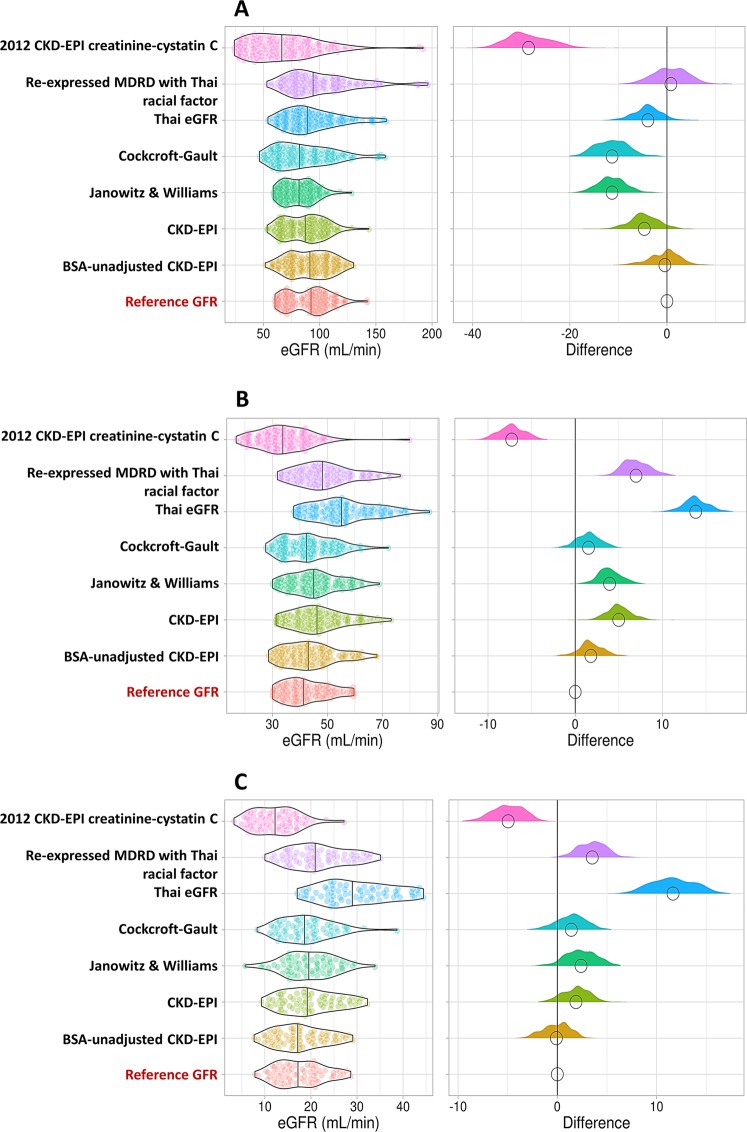
The accuracy of the estimated glomerular filtration rate (eGFR) in cancer patients is very important for dose adjustments of anti-malignancy drugs to reduce toxicities and enhance therapeutic outcomes. Therefore, the performance of eGFR equations, including their bias, precision, and accuracy, was explored in patients with varying stages of chronic kidney disease (CKD) who needed anti-cancer drugs. The reference glomerular filtration rate (GFR) was assessed by the Tc-diethylene triamine penta-acetic acid (Tc-DTPA) plasma clearance method in 320 patients and compared with the GFRs estimated by i) the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, ii) the unadjusted for body surface area (BSA) CKD-EPI equation, iii) the re-expressed Modification of Diet in Renal Disease (MDRD) study equation with the Thai racial factor, iv) the Thai eGFR equation, developed in CKD patients, v) the 2012 CKD-EPI creatinine-cystatin C, vi) the Cockcroft-Gault formula, and vii) the Janowitz and Williams equations for cancer patients. The mean reference GFR was 60.5 ± 33.4 mL/min/1.73 m. The bias (mean error) values for the estimated GFR from the CKD-EPI equation, BSA-unadjusted CKD-EPI equation, re-expressed MDRD study equation with the Thai racial factor, and Thai eGFR, 2012 CKD-EPI creatinine-cystatin-C, Cockcroft-Gault, and Janowitz and Williams equations were -2.68, 1.06, -7.70, -8.73, 13.37, 1.43, and 2.03 mL/min, respectively, the precision (standard deviation of bias) values were 6.89, 6.07, 14.02, 11.54, 20.85, 10.58, and 8.74 mL/min, respectively, and the accuracy (root-mean square error) values were 7.38, 6.15, 15.97, 14.16, 24.74, 10.66, and 8.96 mL/min, respectively. In conclusion, the estimated GFR from the BSA-unadjusted CKD-EPI equation demonstrated the least bias along with the highest precision and accuracy. Further studies on the outcomes of anti-cancer drug dose adjustments using this equation versus the current standard equation will be valuable.
估算肾小球滤过率(eGFR)在癌症患者中的准确性对于调整抗肿瘤药物剂量以降低毒性和提高治疗效果非常重要。因此,在需要抗肿瘤药物的不同慢性肾脏病(CKD)分期的患者中,我们探索了 eGFR 方程的性能,包括其偏差、精密度和准确性。参考肾小球滤过率(GFR)通过 320 例患者的 Tc-二亚乙基三胺五乙酸(Tc-DTPA)血浆清除法评估,并与 i)慢性肾脏病流行病学协作(CKD-EPI)方程、ii)未校正体表面积(BSA)的 CKD-EPI 方程、iii)用泰国种族因素重新表达的改良肾脏病饮食研究(MDRD)方程、iv)泰国 eGFR 方程、v)2012 年 CKD-EPI 肌酐-胱抑素 C、vi) Cockcroft-Gault 公式和 vii)癌症患者的 Janowitz 和 Williams 方程估算的 GFR 进行比较。参考平均 GFR 为 60.5 ± 33.4 mL/min/1.73 m。CKD-EPI 方程、BSA 未校正 CKD-EPI 方程、用泰国种族因素重新表达的 MDRD 研究方程和泰国 eGFR、2012 年 CKD-EPI 肌酐-胱抑素 C、Cockcroft-Gault 和 Janowitz 和 Williams 方程估算的 eGFR 的平均偏差(平均误差)值分别为-2.68、1.06、-7.70、-8.73、13.37、1.43 和 2.03 mL/min,精密度(偏差标准差)值分别为 6.89、6.07、14.02、11.54、20.85、10.58 和 8.74 mL/min,准确性(均方根误差)值分别为 7.38、6.15、15.97、14.16、24.74、10.66 和 8.96 mL/min。总之,BSA 未校正 CKD-EPI 方程估算的 eGFR 具有最小的偏差,同时具有最高的精密度和准确性。使用该方程与当前标准方程对癌症药物剂量调整的结果进行进一步研究将是有价值的。