Department of Neurology, Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Centre of Expertise for Parkinson & Movement Disorders, Nijmegen, The Netherlands.
Department of Neurology, University of São Paulo, Movement Disorder Center, São Paulo, Brazil.
J Parkinsons Dis. 2020;10(1):333-346. doi: 10.3233/JPD-191752.
Balance impairment in Parkinson's disease (PD) improves only partially with dopaminergic medication. Therefore, non-pharmacological interventions such as physiotherapy are important elements in clinical management. External cues are often applied to improve gait, but their effects on balance control are unclear.
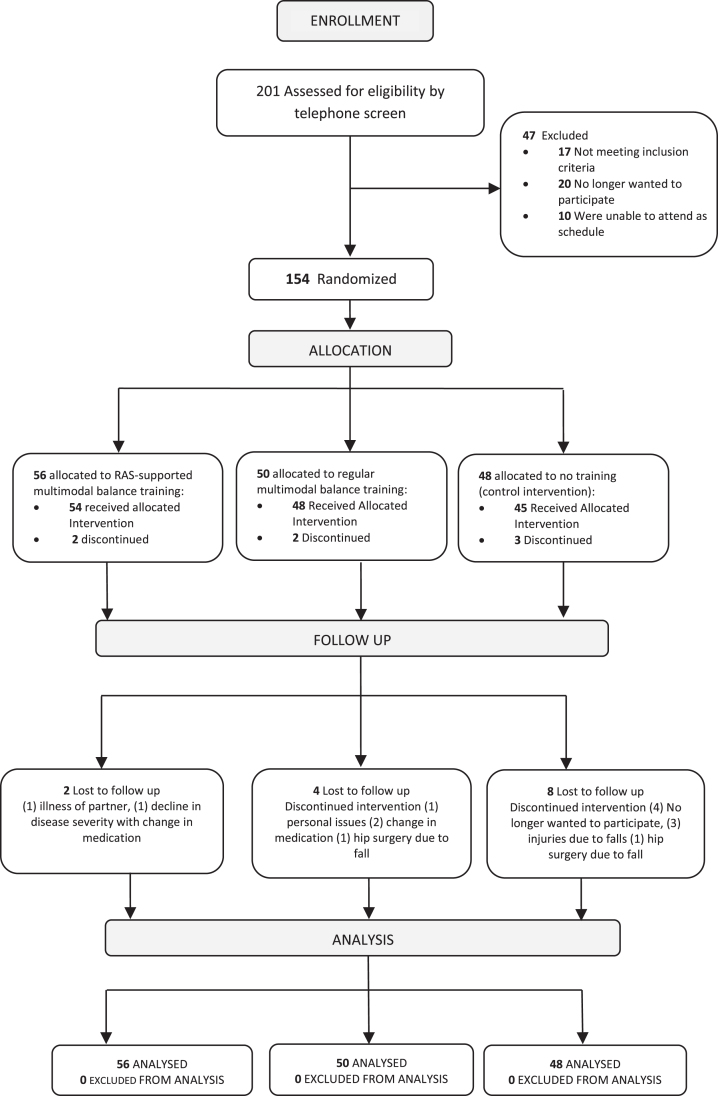
OBJECTIVE/METHODS: We performed a prospective, single-blind, randomized clinical trial to study the effectiveness of balance training with and without rhythmical auditory cues. We screened 201 volunteers by telephone; 154 were assigned randomly into three groups: (1) multimodal balance training supported by rhythmical auditory stimuli (n = 56) (RAS-supported multimodal balance training); (2) regular multimodal balance training without rhythmical auditory stimuli (n = 50); and (3) control intervention involving a general education program (n = 48). Training was performed for 5 weeks, two times/week. Linear mixed models were used for all outcomes. Primary outcome was the Mini-BESTest (MBEST) score immediately after the training period. Assessments were performed by a single, blinded assessor at baseline, immediately post intervention, and after one and 6-months follow-up.
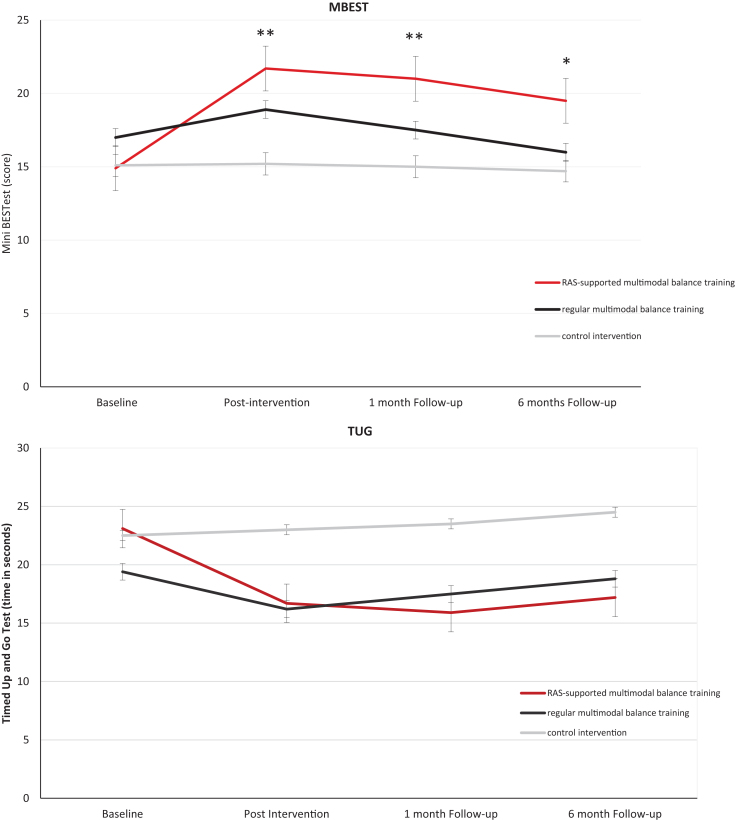
Immediately post intervention, RAS-supported multimodal balance training was more effective than regular multimodal balance training on MBEST (difference 3.5 (95% Confidence Interval (CI) 2.2; 4.8)), p < 0.001). Patients allocated to both active interventions improved compared to controls (MBEST estimated mean difference versus controls 6.6 (CI 5.2; 8.0), p < 0.001 for RAS-supported multimodal balance training; and 3.0 (CI 2.7; 5.3), p < 0.001 for regular multimodal balance training). Improvements were retained at one-month follow-up for both active interventions, but only the RAS-supported multimodal balance training group maintained its improvement at 6 months.
Both RAS-supported multimodal balance training and regular multimodal balance training improve balance, but RAS-supported multimodal balance training-adding rhythmical auditory cues to regular multimodal balance training-has greater and more sustained effects.
帕金森病(PD)患者的平衡障碍仅部分通过多巴胺能药物治疗得到改善。因此,非药物干预,如物理治疗,是临床管理的重要组成部分。外部提示通常用于改善步态,但它们对平衡控制的影响尚不清楚。
目的/方法:我们进行了一项前瞻性、单盲、随机临床试验,研究了有节奏的听觉提示和无节奏的听觉提示对平衡训练的有效性。我们通过电话对 201 名志愿者进行了筛查;154 名志愿者被随机分配到三组:(1)有节奏的听觉刺激支持的多模态平衡训练(n=56)(RAS 支持的多模态平衡训练);(2)无节奏的听觉刺激的常规多模态平衡训练(n=50);和(3)涉及一般教育计划的对照干预(n=48)。训练每周进行两次,共 5 周。线性混合模型用于所有结果。主要结局指标是训练期结束后即刻的 Mini-BESTest(MBEST)评分。在基线、干预后即刻、1 个月和 6 个月随访时,由一位单一、盲法评估者进行评估。
干预后即刻,RAS 支持的多模态平衡训练在 MBEST 上比常规多模态平衡训练更有效(差异 3.5(95%置信区间(CI)2.2;4.8),p<0.001)。接受两种积极干预的患者与对照组相比有所改善(与对照组相比,RAS 支持的多模态平衡训练的 MBEST 估计平均差异为 6.6(CI 5.2;8.0),p<0.001;常规多模态平衡训练为 3.0(CI 2.7;5.3),p<0.001)。两种积极干预在 1 个月随访时都保持了改善,但只有 RAS 支持的多模态平衡训练组在 6 个月时保持了改善。
有节奏的听觉提示支持的多模态平衡训练和常规多模态平衡训练都能改善平衡,但有节奏的听觉提示支持的多模态平衡训练(在常规多模态平衡训练中加入节奏性听觉提示)效果更大且更持久。