March Sonja, Donovan Caroline L, Baldwin Sarah, Ford Martelle, Spence Susan H
University of Southern Queensland, School of Psychology and Counselling and Centre for Health, Informatics and Economics Research, Springfield, QLD 4300, Australia.
Griffith University, School of Applied Psychology, Mt Gravatt, QLD, Australia.
Internet Interv. 2019 Sep 10;18:100281. doi: 10.1016/j.invent.2019.100281. eCollection 2019 Dec.
There are a lack of clear guidelines for the dissemination of Internet-based cognitive behaviour therapy (ICBT) for childhood and adolescent anxiety in routine care. While self-guided ICBT has greater reach than therapist-guided ICBT, it is plagued by problems of low program adherence and many young people are not successfully treated. It is important that we identify models of ICBT that are accessible, but provide the right support, at the right time to those who need it. Stepped-care models of ICBT offer one potential solution.
This case study examined the application of stepped-care within an ICBT intervention for childhood and adolescent anxiety, in which young people were stepped up from self-guided to therapist-guided ICBT.
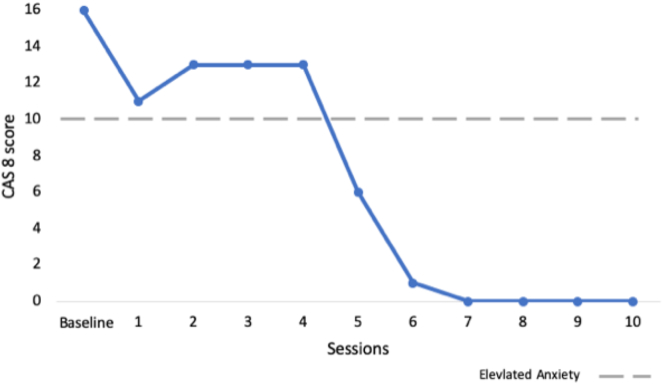
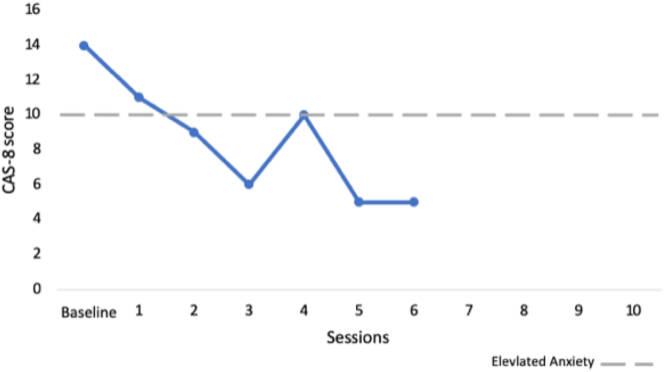
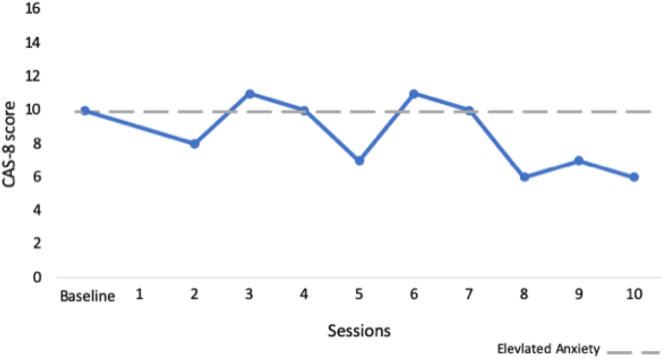
Three case studies are presented and include young males (aged 11-12 years) who participated in BRAVE Stepped-Care, a new ICBT program incorporating two treatment steps: Step 1 - five sessions of self-guided ICBT and Step 2 - five sessions of therapist-guided ICBT. Participants completed diagnostic assessments at pre- and post-treatment, along with a battery of self-report questionnaires. Step-up requirements were determined at a mid-treatment assessment. Treatment response was determined by change on diagnostic severity and presence of diagnosis and changes in self-reported anxiety symptoms (through T-scores and Reliable Change Indices).
In-depth examination of the three case studies showed that decisions to step-up from Step 1 to Step 2 were complex and required consideration of program engagement and adherence, as well as changes on self-reported anxiety, behavioural indicators of anxiety and parent perspectives. Results showed that non-responders at mid-treatment who were stepped-up to therapist-guided ICBT after Step 1 were able to increase engagement and response to treatment in Step 2, such that they were free of their primary anxiety diagnosis at post-treatment.
The findings highlight the importance of early assessment of engagement and non-response within self-guided ICBT programs for youth anxiety and the positive changes that can subsequently occur when therapist-guidance is introduced mid-treatment for non-responders. The efficacy of stepped-care ICBT models needs to be confirmed in larger randomised controlled trials.
在常规护理中,针对儿童和青少年焦虑症的基于互联网的认知行为疗法(ICBT)的传播缺乏明确的指导方针。虽然自我指导的ICBT比治疗师指导的ICBT覆盖面更广,但它受到程序依从性低的问题困扰,许多年轻人未能得到成功治疗。重要的是,我们要确定那些易于获取的ICBT模式,能在恰当的时间为有需要的人提供恰当的支持。ICBT的阶梯式护理模式提供了一种潜在的解决方案。
本案例研究考察了阶梯式护理在针对儿童和青少年焦虑症的ICBT干预中的应用,在该干预中,年轻人从自我指导的ICBT逐步升级到治疗师指导的ICBT。
呈现了三个案例研究,包括参与BRAVE阶梯式护理的年轻男性(11 - 12岁),这是一个新的ICBT项目,包含两个治疗步骤:步骤1 - 五节自我指导的ICBT课程,步骤2 - 五节治疗师指导的ICBT课程。参与者在治疗前和治疗后完成诊断评估,以及一系列自我报告问卷。在治疗中期评估时确定升级要求。治疗反应通过诊断严重程度的变化、诊断的存在以及自我报告焦虑症状的变化(通过T分数和可靠变化指数)来确定。
对这三个案例研究的深入检查表明,从步骤1升级到步骤2的决定很复杂,需要考虑项目参与度和依从性,以及自我报告焦虑的变化、焦虑的行为指标和家长的观点。结果显示,在治疗中期没有反应的人在步骤1后升级到治疗师指导的ICBT,能够在步骤2中提高参与度和对治疗的反应,从而在治疗后摆脱主要的焦虑诊断。
研究结果强调了在针对青少年焦虑症的自我指导ICBT项目中早期评估参与度和无反应情况的重要性,以及在治疗中期对无反应者引入治疗师指导后随后可能发生的积极变化。阶梯式护理ICBT模式的疗效需要在更大规模的随机对照试验中得到证实。