Division of Epidemiology, Department of Health Sciences Research, Mayo Clinic, Rochester, MN.
Division of Health Policy and Management, School of Public Health, University of Minnesota, Minneapolis, MN.
Transplantation. 2020 Nov;104(11):2383-2392. doi: 10.1097/TP.0000000000003131.
Despite extensive evaluation processes to determine candidacy for kidney transplantation, variability in graft failure exists. The role of patient socioeconomic status (SES) in transplantation outcomes is poorly understood because of limitations of conventional SES measures.
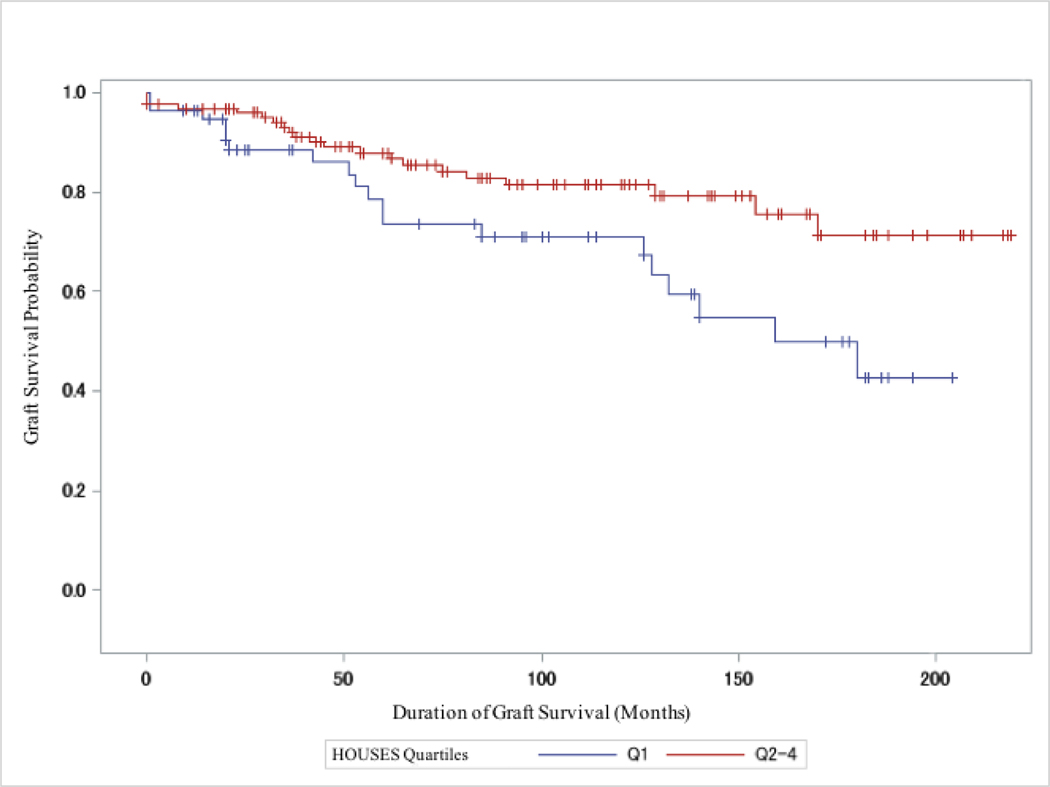
This population-based retrospective cohort study assessed whether a validated objective and individual-level housing-based SES index (HOUSES) would serve as a predictive tool for graft failure in patients (n = 181) who received a kidney transplant in Olmsted County, MN (January 1, 1998 to December 8, 2016). Associations were assessed between HOUSES (quartiles: Q1 [lowest] to Q4 [highest]) and graft failure until last follow-up date (December 31, 2016) using Cox proportional hazards. The mean age (SD) was 46.1 (17.2) years, 109 (60.2%) were male, 113 (62.4%) received a living kidney donor transplant, and 40 (22.1%) had a graft failure event.
Compared with Q1, patients with higher HOUSES (Q2-Q4) had significantly lower graft failure rates (adjusted hazard ratio, 0.47; 95% confidence interval, 0.24-0.92; P < 0.029), controlling for age, sex, race, previous kidney transplantation, and donor type.
Although criteria for kidney transplant recipients are selective, patients with higher HOUSES had lower graft failure rates. Thus, HOUSES may enable transplantation programs to identify a target group for improving kidney transplantation outcomes.
尽管有广泛的评估过程来确定肾移植的候选资格,但移植物衰竭的情况存在差异。由于传统社会经济地位(SES)衡量标准的局限性,患者 SES 状况在移植结果中的作用尚不清楚。
本基于人群的回顾性队列研究评估了经过验证的客观和个体层面基于住房的 SES 指数(HOUSES)是否可作为明尼苏达州奥姆斯特德县(1998 年 1 月 1 日至 2016 年 12 月 8 日)接受肾移植的患者(n=181)发生移植物衰竭的预测工具。使用 Cox 比例风险评估 HOUSES(四分位数:Q1[最低]至 Q4[最高])与直至最后随访日期(2016 年 12 月 31 日)的移植物衰竭之间的相关性。平均年龄(SD)为 46.1(17.2)岁,109 例(60.2%)为男性,113 例(62.4%)接受活体供肾移植,40 例(22.1%)发生移植物衰竭事件。
与 Q1 相比,HOUSES 较高的患者(Q2-Q4)移植物衰竭率显著降低(调整后的危险比,0.47;95%置信区间,0.24-0.92;P<0.029),同时控制了年龄、性别、种族、既往肾移植和供体类型。
尽管肾移植受者的标准是选择性的,但 HOUSES 较高的患者移植物衰竭率较低。因此,HOUSES 可能使移植计划能够确定一个改善肾移植结果的目标群体。