Bose Corporation, Framingham, MA, USA.
Roxelyn and Richard Pepper Department of Communication Sciences and Disorders, Northwestern University, Evanston, IL, USA.
Trends Hear. 2020 Jan-Dec;24:2331216519900589. doi: 10.1177/2331216519900589.
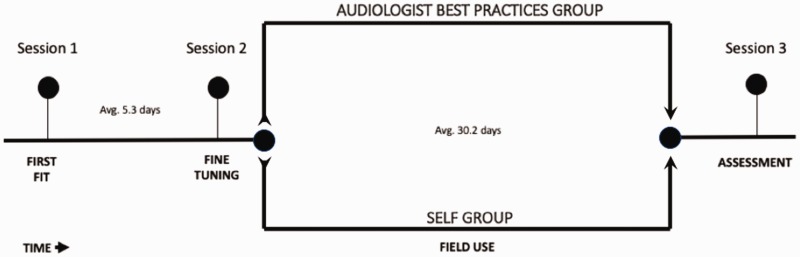
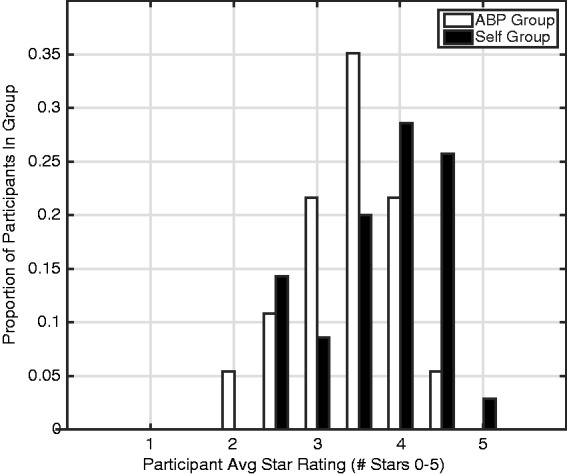
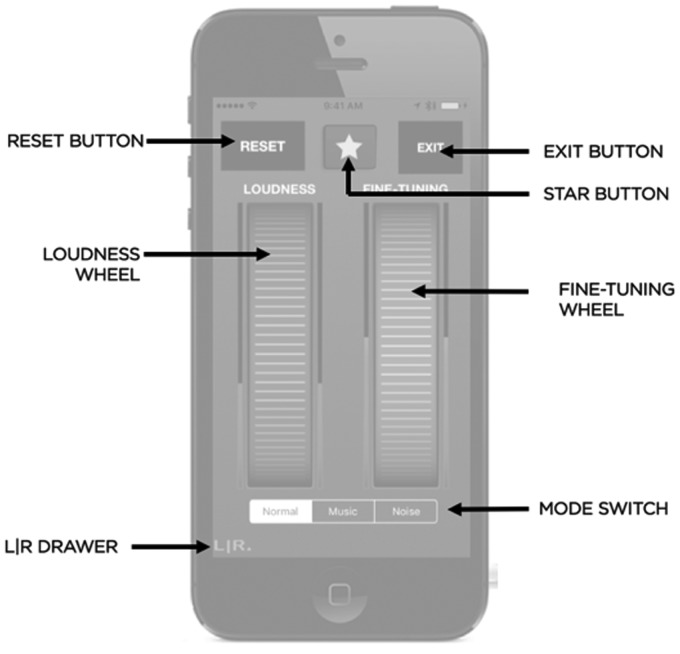
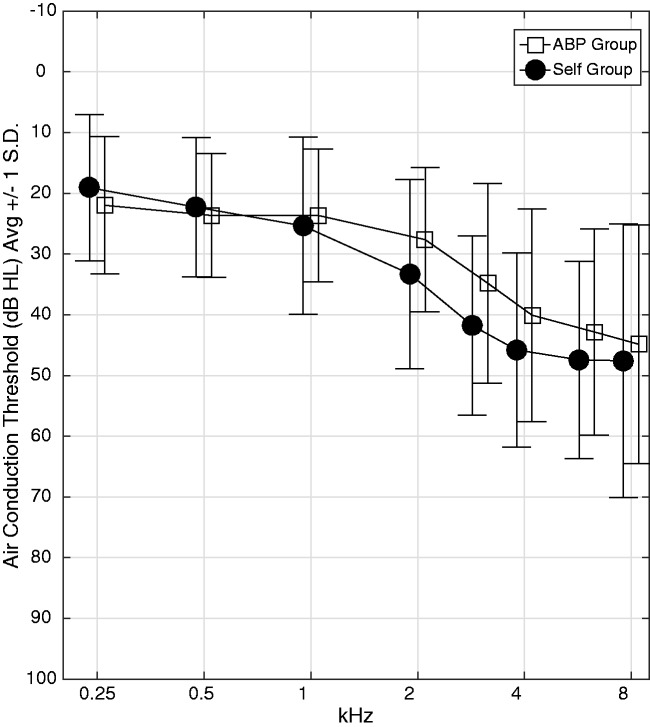
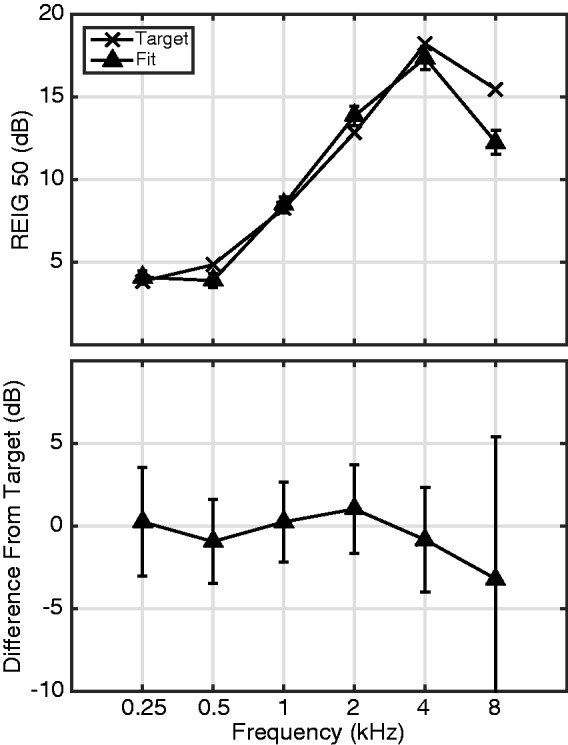
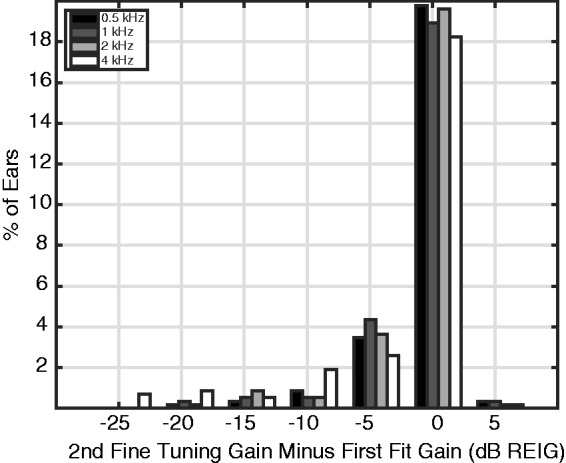
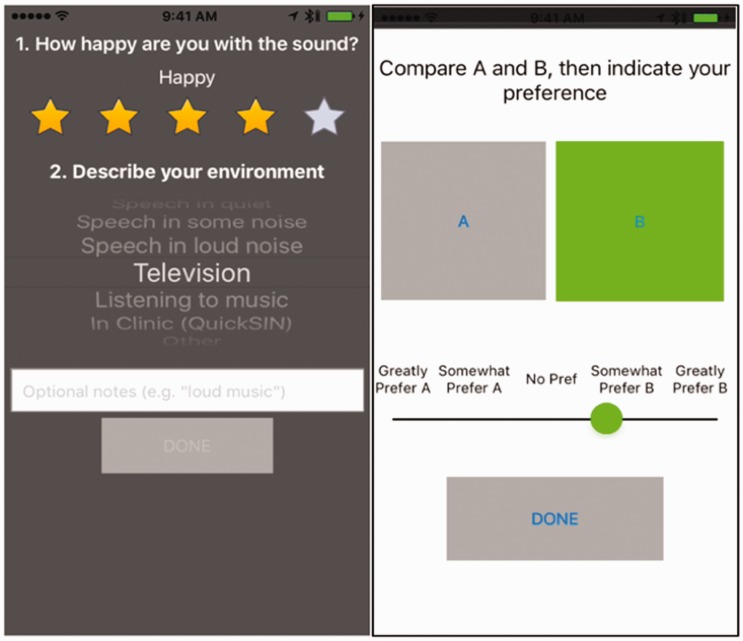
In common practice, hearing aids are fitted by a clinician who measures an audiogram and uses it to generate prescriptive gain and output targets. This report describes an alternative method where users select their own signal processing parameters using an interface consisting of two wheels that optimally map to simultaneous control of gain and compression in each frequency band. The real-world performance of this approach was evaluated via a take-home field trial. Participants with hearing loss were fitted using clinical best practices (audiogram, fit to target, real-ear verification, and subsequent fine tuning). Then, in their everyday lives over the course of a month, participants either selected their own parameters using this new interface (Self group; n = 38) or used the parameters selected by the clinician with limited control (Audiologist Best Practices Group; n = 37). On average, the gain selected by the Self group was within 1.8 dB overall and 5.6 dB per band of that selected by the audiologist. Participants in the Self group reported better sound quality than did those in the Audiologist Best Practices group. In blind sound quality comparisons conducted in the field, participants in the Self group slightly preferred the parameters they selected over those selected by the clinician. Finally, there were no differences between groups in terms of standard clinical measures of hearing aid benefit or speech perception in noise. Overall, the results indicate that it is possible for users to select effective amplification parameters by themselves using a simple interface that maps to key hearing aid signal processing parameters.
在常规实践中,助听器是由临床医生通过测量听力图并使用该听力图生成处方增益和输出目标来适配的。本报告描述了一种替代方法,用户使用由两个轮子组成的界面自行选择信号处理参数,这两个轮子最佳地映射到每个频带中增益和压缩的同时控制。通过一项家庭实地试验评估了这种方法的实际性能。使用临床最佳实践(听力图、目标适配、真耳验证和后续微调)为听力损失患者进行适配。然后,在一个月的日常生活中,参与者使用新界面自行选择参数(自我组;n = 38)或使用临床医生选择的参数(助听器最佳实践组;n = 37)进行有限控制。平均而言,自我组选择的增益在整体上在 1.8dB 以内,每个频带的增益在 5.6dB 以内,均低于临床医生选择的增益。自我组的参与者报告说声音质量比助听器最佳实践组的参与者好。在现场进行的盲听质量比较中,自我组的参与者略微更喜欢他们自己选择的参数,而不是临床医生选择的参数。最后,在助听器获益和噪声下言语感知的标准临床测量方面,两组之间没有差异。总体而言,结果表明,用户可以使用简单的界面自行选择有效的放大参数,该界面映射到关键的助听器信号处理参数。