Department of Epidemiology and Biostatistics, Institute of Basic Medical Sciences Chinese Academy of Medical Sciences, School of Basic Medicine Peking Union Medical College, Beijing, 100005, China.
Department of Critical Care Medicine, The Second People's Hospital of Shenzhen & First Affiliated Hospital of Shenzhen University, Health Science Center, Shenzhen, 518035, China.
Infect Dis Poverty. 2020 Feb 5;9(1):14. doi: 10.1186/s40249-020-0623-8.
Despite the availability of free tuberculosis (TB) diagnosis and treatment, TB care still generates substantial costs that push people into poverty. We investigated out-of-pocket (OOP) payments for TB care and assessed the resulting economic burden and economic consequences for those with varying levels of household income in eastern China.
A cross-sectional study was conducted among TB patients in the national TB programme networks in eastern China. TB-related direct OOP costs, time loss, and coping strategies were investigated across households in different economic strata. Analysis of Variance was used to examine the differences in various costs, and Kruskal-Wallis tests were used to compare the difference in total costs as a percentage of annual household income.
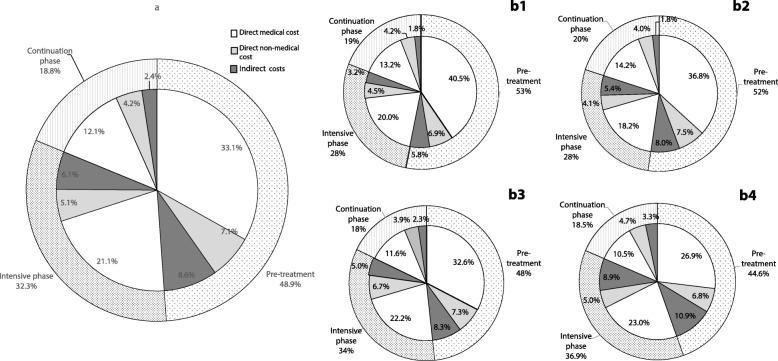
Among 435 patients, the mean OOP total costs of TB care were USD 2389.5. In the lower-income quartile, OOP payments were lower, but costs as a percentage of reported annual household income were higher. Medical costs and costs prior to treatment accounted for 66.4 and 48.9% of the total costs, respectively. The lower the household income was, the higher the proportion of medical costs to total costs before TB treatment, but the lower the proportion of medical costs patients spent in the intensive phase. TB care caused 25.8% of TB-affected households to fall below the poverty line and caused the poverty gap (PG) to increase by United States Dollar (USD) 145.6. Patients in the poorest households had the highest poverty headcount ratio (70.2%) and PG (USD 236.1), but those in moderately poor households had the largest increase in the poverty headcount ratio (36.2%) and PG (USD 177.8) due to TB care. Patients from poor households were more likely to borrow money to cope with the costs of TB care; however, there were fewer social consequences, except for food insecurity, in poor households.
Medical and pretreatment costs lead to high costs of TB care, especially among patients from the poorest households. It is necessary to train health system staff in general hospitals to promptly identify and refer TB patients. Pro-poor programmes are also needed to protect TB patients from the medical poverty trap.
尽管结核病(TB)的诊断和治疗是免费的,但结核病的护理仍会产生大量费用,使人们陷入贫困。我们调查了结核病护理的自付费用,并评估了中国东部不同收入家庭的经济负担和经济后果。
在中国东部国家结核病规划网络中,对结核病患者进行了一项横断面研究。调查了不同经济阶层家庭的结核病相关直接自付费用、时间损失和应对策略。方差分析用于检查各种费用的差异,Kruskal-Wallis 检验用于比较总费用占家庭年收入的百分比差异。
在 435 名患者中,结核病护理的平均自付总费用为 2389.5 美元。在低收入四分位数中,自付费用较低,但费用占报告的年度家庭收入的百分比较高。医疗费用和治疗前费用分别占总费用的 66.4%和 48.9%。家庭收入越低,结核病治疗前的医疗费用占总费用的比例越高,但结核病治疗强化期患者的医疗费用比例越低。结核病护理使 25.8%的受结核病影响的家庭陷入贫困线以下,使贫困差距(PG)增加 145.6 美元。最贫困家庭的贫困人口比例(70.2%)和 PG(145.6 美元)最高,但由于结核病护理,中等贫困家庭的贫困人口比例(36.2%)和 PG(177.8 美元)增幅最大。来自贫困家庭的患者更有可能借钱来支付结核病护理费用;然而,除了粮食不安全之外,贫困家庭的社会后果较少。
医疗和治疗前费用导致结核病护理费用高昂,尤其是来自最贫困家庭的患者。有必要培训综合医院的卫生系统工作人员,以便及时识别和转介结核病患者。还需要制定扶贫方案,以防止结核病患者陷入医疗贫困陷阱。