Health Services and Policy Research Group, Institute for Health Sciences in Aragon (IACS), Zaragoza, Spain.
Network for Health Services Research in Chronic Patients (REDISSEC), Madrid, Spain.
PLoS One. 2020 Feb 6;15(2):e0228425. doi: 10.1371/journal.pone.0228425. eCollection 2020.
Hospital performance, presented as the comparison of average measurements, dismisses that hospital outcomes may vary across types of patients. We aim at drawing out the relevance of accounting for patient heterogeneity when reporting on hospital performance.
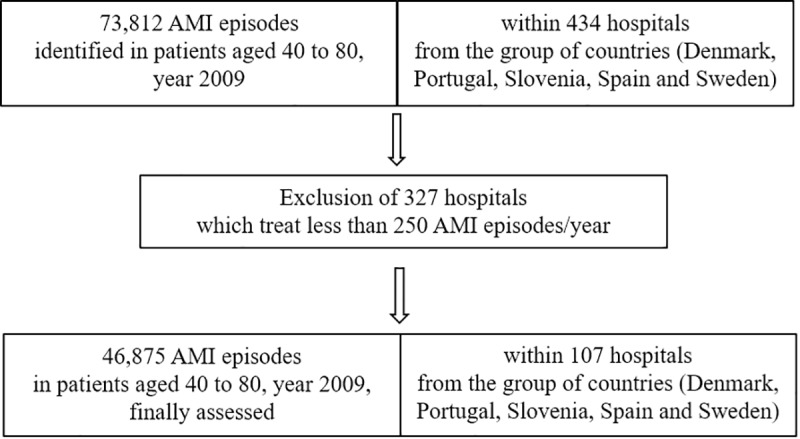
An observational study on administrative data from virtually all 2009 hospital admissions for Acute Myocardial Infarction (AMI) discharged in Denmark, Portugal, Slovenia, Spain, and Sweden. Hospital performance was proxied using in-hospital risk-adjusted mortality. Multilevel Regression Modelling (MLRM) was used to assess differences in hospital performance, comparing the estimates of random intercept modelling (capturing hospital general contextual effects (GCE)), and random slope modelling (capturing hospital contextual effects for patients with and without congestive heart failure -CHF). The weighted Kappa Index (KI) was used to assess the agreement between performance estimates.
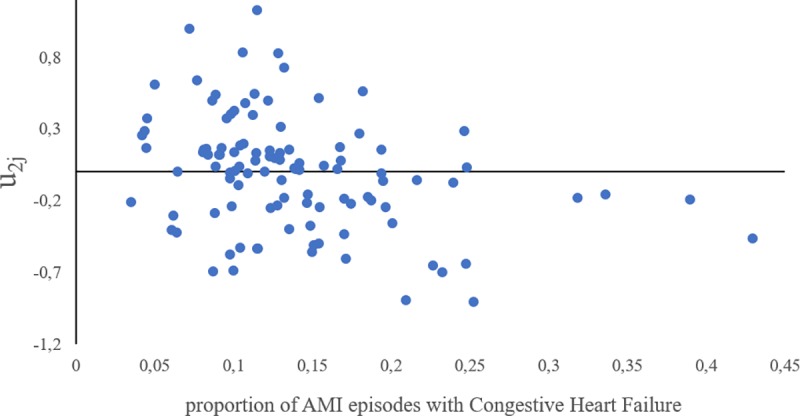
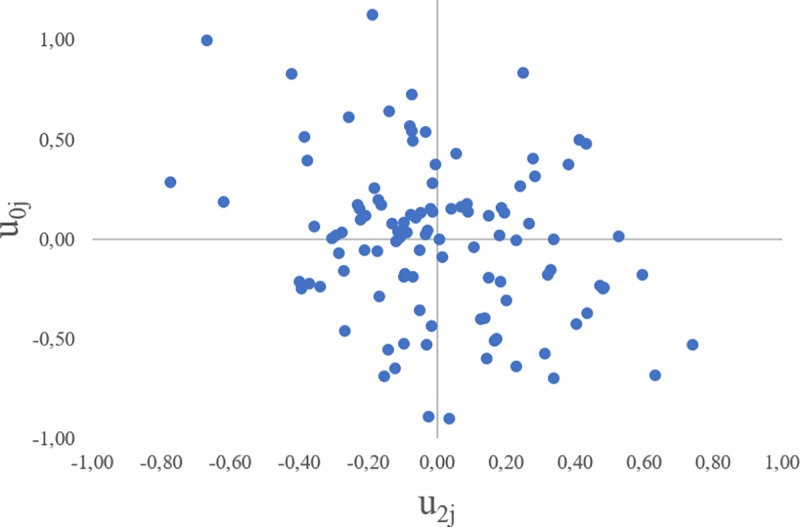
We analysed 46,875 admissions of AMI, 6,314 with coexistent CHF, discharged from 107 hospitals. The overall in-hospital mortality rate was 5.2%, ranging from 4% in Sweden to 6.9% in Portugal. The MLRM with random slope outperformed the model with only random intercept, highlighting a much higher GCE in CHF patients [VPC = 8.34 (CI95% 4.94 to 13.03) and MOR = 1.69 (CI95% 1.62 to 2.21) vs. VPC = 3.9 (CI95% 2.4 to 5.9), MOR of 1.42 (CI95% 1.31 to 1.54) without CHF]. No agreement was observed between estimates [KI = -0,02 (CI95% -0,08 to 0.04].
The different GCE in AMI patients with and without CHF, along with the lack of agreement in estimates, suggests that accounting for patient heterogeneity is required to adequately characterize and report on hospital performance.
医院绩效以平均指标的比较呈现,忽略了医院结果可能因患者类型而异。我们旨在指出在报告医院绩效时考虑患者异质性的重要性。
这是一项基于丹麦、葡萄牙、斯洛文尼亚、西班牙和瑞典 2009 年所有急性心肌梗死(AMI)住院患者出院后行政数据的观察性研究。使用住院风险调整死亡率来代理医院绩效。多水平回归模型(MLRM)用于评估医院绩效的差异,比较随机截距模型(捕捉医院一般背景效应(GCE))和随机斜率模型(捕捉有无充血性心力衰竭(CHF)的患者的医院背景效应)的估计值。使用加权 Kappa 指数(KI)评估绩效估计值之间的一致性。
我们分析了 46875 例 AMI 住院患者,其中 6314 例合并 CHF,来自 107 家医院。总的院内死亡率为 5.2%,范围从瑞典的 4%到葡萄牙的 6.9%。具有随机斜率的 MLRM 优于仅具有随机截距的模型,突出了 CHF 患者中更高的 GCE [预测百分比变化(VPC)= 8.34(95%CI95% 4.94 至 13.03)和平均比值比(MOR)= 1.69(95%CI95% 1.62 至 2.21)与 VPC = 3.9(95%CI95% 2.4 至 5.9),MOR 为 1.42(95%CI95% 1.31 至 1.54)无 CHF]。估计值之间没有观察到一致性[KI = -0.02(95%CI95% -0.08 至 0.04)]。
AMI 患者中 CHF 患者和无 CHF 患者的 GCE 存在差异,且估计值之间缺乏一致性,这表明需要考虑患者异质性来充分描述和报告医院绩效。