Department of Epidemiology and Preventive Medicine, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, Australia.
BMC Med Res Methodol. 2012 Mar 12;12:28. doi: 10.1186/1471-2288-12-28.
Marginal and multilevel logistic regression methods can estimate associations between hospital-level factors and patient-level 30-day mortality outcomes after cardiac surgery. However, it is not widely understood how the interpretation of hospital-level effects differs between these methods.
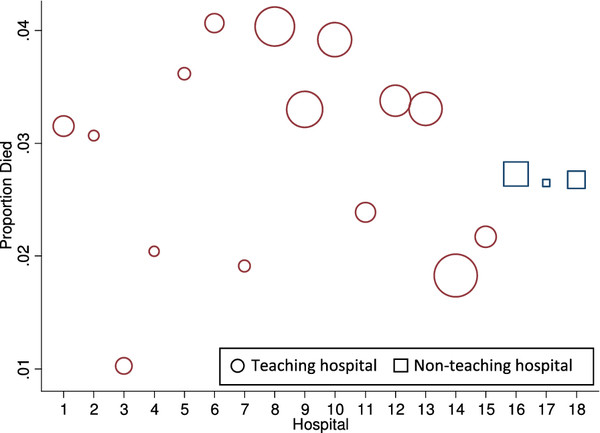
The Australasian Society of Cardiac and Thoracic Surgeons (ASCTS) registry provided data on 32,354 patients undergoing cardiac surgery in 18 hospitals from 2001 to 2009. The logistic regression methods related 30-day mortality after surgery to hospital characteristics with concurrent adjustment for patient characteristics.
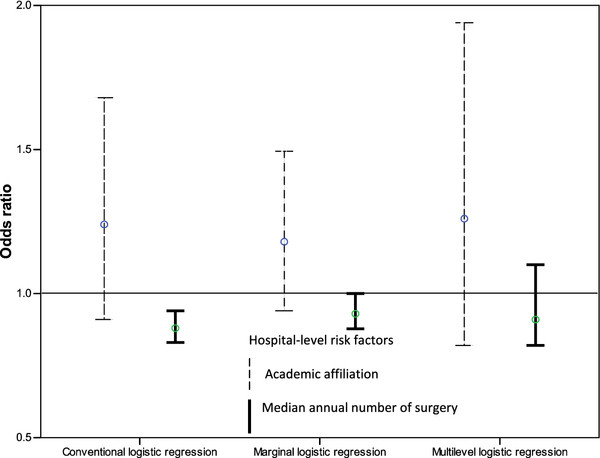
Hospital-level mortality rates varied from 1.0% to 4.1% of patients. Ordinary, marginal and multilevel regression methods differed with regard to point estimates and conclusions on statistical significance for hospital-level risk factors; ordinary logistic regression giving inappropriately narrow confidence intervals. The median odds ratio, MOR, from the multilevel model was 1.2 whereas ORs for most patient-level characteristics were of greater magnitude suggesting that unexplained between-hospital variation was not as relevant as patient-level characteristics for understanding mortality rates. For hospital-level characteristics in the multilevel model, 80% interval ORs, IOR-80%, supplemented the usual ORs from the logistic regression. The IOR-80% was (0.8 to 1.8) for academic affiliation and (0.6 to 1.3) for the median annual number of cardiac surgery procedures. The width of these intervals reflected the unexplained variation between hospitals in mortality rates; the inclusion of one in each interval suggested an inability to add meaningfully to explaining variation in mortality rates.
Marginal and multilevel models take different approaches to account for correlation between patients within hospitals and they lead to different interpretations for hospital-level odds ratios.
边缘和多层次逻辑回归方法可以估计医院水平因素与心脏手术后患者 30 天死亡率之间的关联。然而,人们并不广泛了解这两种方法在解释医院水平效应方面有何不同。
澳大利亚心脏和胸外科医师协会(ASCTS)注册中心提供了 2001 年至 2009 年间 18 家医院 32354 例心脏手术患者的数据。逻辑回归方法将手术后 30 天的死亡率与医院特征相关联,并同时调整患者特征。
医院水平死亡率从 1.0%到 4.1%的患者不等。普通、边缘和多层次回归方法在医院水平危险因素的点估计和统计显著性结论方面存在差异;普通逻辑回归给出了不适当的置信区间。来自多层次模型的中位数优势比,MOR,为 1.2,而大多数患者水平特征的 OR 则更大,这表明无法解释的医院间差异对于理解死亡率并不像患者水平特征那样重要。在多层次模型中,80%的区间 OR,IOR-80%,补充了逻辑回归中通常的 OR。MOR-80%为学术隶属关系(0.8 至 1.8)和中位数每年心脏手术数量(0.6 至 1.3)。这些区间的宽度反映了死亡率方面医院间无法解释的差异;在每个区间中包含一个,表明无法有意义地增加对死亡率变异的解释。
边缘和多层次模型采取不同的方法来解释医院内患者之间的相关性,并且导致对医院水平优势比的不同解释。