Division of Infectious Diseases, Department of Medicine, Solna (MedS), Karolinska Institutet, Stockholm, Sweden
Department of Infectious Diseases, Karolinska University Hospital, Stockholm, Sweden.
BMJ Qual Saf. 2020 Sep;29(9):735-745. doi: 10.1136/bmjqs-2019-010123. Epub 2020 Feb 6.
Surveillance of sepsis incidence is important for directing resources and evaluating quality-of-care interventions. The aim was to develop and validate a fully-automated Sepsis-3 based surveillance system in non-intensive care wards using electronic health record (EHR) data, and demonstrate utility by determining the burden of hospital-onset sepsis and variations between wards.
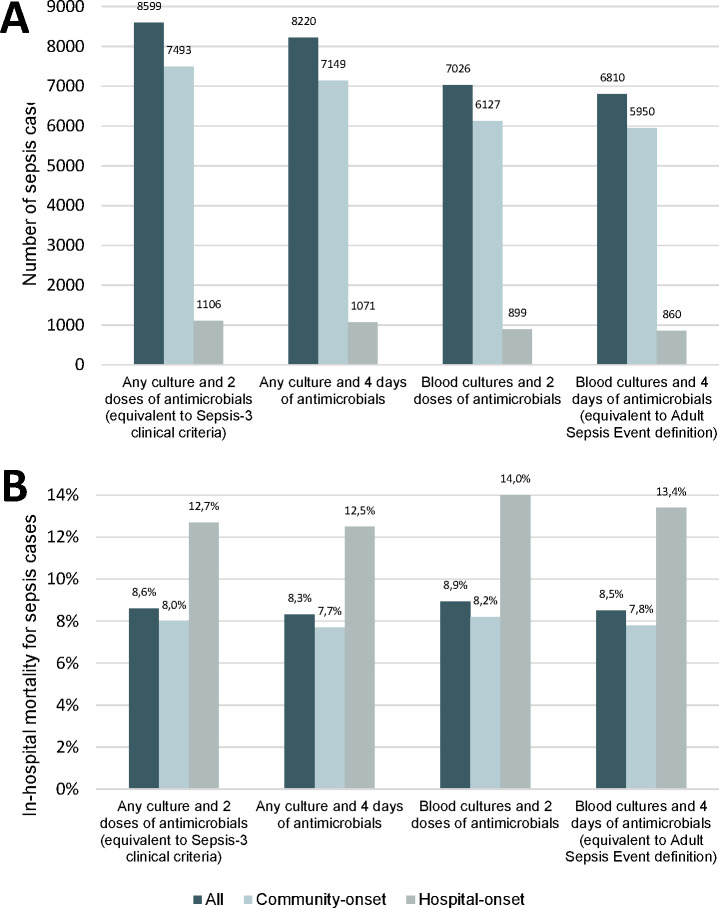
A rule-based algorithm was developed using EHR data from a cohort of all adult patients admitted at an academic centre between July 2012 and December 2013. Time in intensive care units was censored. To validate algorithm performance, a stratified random sample of 1000 hospital admissions (674 with and 326 without suspected infection) was classified according to the Sepsis-3 clinical criteria (suspected infection defined as having any culture taken and at least two doses of antimicrobials administered, and an increase in Sequential Organ Failure Assessment (SOFA) score by 2 points) and the likelihood of infection by physician medical record review.
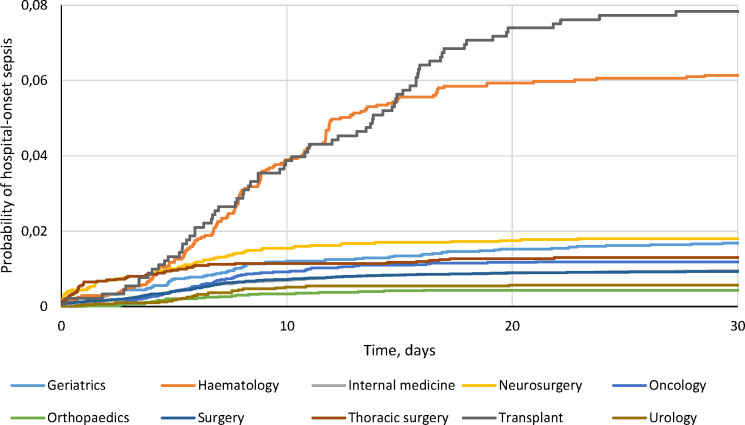
In total 82 653 hospital admissions were included. The Sepsis-3 clinical criteria determined by physician review were met in 343 of 1000 episodes. Among them, 313 (91%) had possible, probable or definite infection. Based on this reference, the algorithm achieved sensitivity 0.887 (95% CI: 0.799 to 0.964), specificity 0.985 (95% CI: 0.978 to 0.991), positive predictive value 0.881 (95% CI: 0.833 to 0.926) and negative predictive value 0.986 (95% CI: 0.973 to 0.996). When applied to the total cohort taking into account the sampling proportions of those with and without suspected infection, the algorithm identified 8599 (10.4%) sepsis episodes. The burden of hospital-onset sepsis (>48 hour after admission) and related in-hospital mortality varied between wards.
A fully-automated Sepsis-3 based surveillance algorithm using EHR data performed well compared with physician medical record review in non-intensive care wards, and exposed variations in hospital-onset sepsis incidence between wards.
对脓毒症发病率进行监测对于指导资源分配和评估医疗质量干预措施非常重要。本研究旨在使用电子病历(EHR)数据开发和验证一种完全基于脓毒症-3 标准的非重症监护病房监测系统,并通过确定医院获得性脓毒症的负担和病房之间的差异来展示其实用性。
使用 2012 年 7 月至 2013 年 12 月期间在一家学术中心住院的所有成年患者队列的 EHR 数据开发了一个基于规则的算法。将 ICU 入住时间作为截尾数据。为了验证算法的性能,对 1000 例住院患者(326 例无疑似感染,674 例有疑似感染)进行了分层随机抽样,并根据脓毒症-3 临床标准(疑似感染定义为至少采集了一次培养物,并使用了至少两种剂量的抗生素,以及序贯器官衰竭评估(SOFA)评分增加 2 分)和医生病历审查确定的感染可能性进行分类。
共纳入 82653 例住院患者。1000 例患者中,医生审查确定符合脓毒症-3 临床标准的有 343 例。其中,313 例(91%)存在可能、很可能或确定的感染。基于该参考标准,该算法的灵敏度为 0.887(95%CI:0.799 至 0.964),特异性为 0.985(95%CI:0.978 至 0.991),阳性预测值为 0.881(95%CI:0.833 至 0.926),阴性预测值为 0.986(95%CI:0.973 至 0.996)。将该算法应用于考虑疑似感染患者和无疑似感染患者抽样比例的总队列时,共识别出 8599 例(10.4%)脓毒症病例。不同病房之间医院获得性脓毒症(入院后超过 48 小时)的负担和相关院内死亡率存在差异。
在非重症监护病房中,使用 EHR 数据的完全基于脓毒症-3 标准的监测算法与医生病历审查相比表现良好,并揭示了不同病房之间医院获得性脓毒症发生率的差异。