Department of Neurology, Massachusetts General Hospital, Boston, MA, USA.
The Mount Sinai Hospital, New York, NY, USA.
Neurocrit Care. 2020 Oct;33(2):479-490. doi: 10.1007/s12028-019-00911-4.
In critical care settings, electroencephalography (EEG) with reduced number of electrodes (reduced montage EEG, rm-EEG) might be a timely alternative to the conventional full montage EEG (fm-EEG). However, past studies have reported variable accuracies for detecting seizures using rm-EEG. We hypothesized that the past studies did not distinguish between differences in sensitivity from differences in classification of EEG patterns by different readers. The goal of the present study was to revisit the diagnostic value of rm-EEG when confounding issues are accounted for.
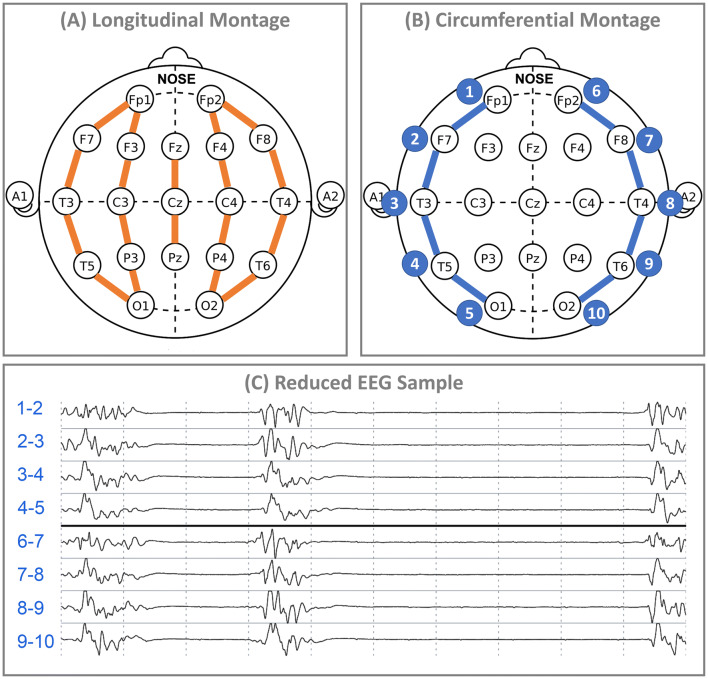
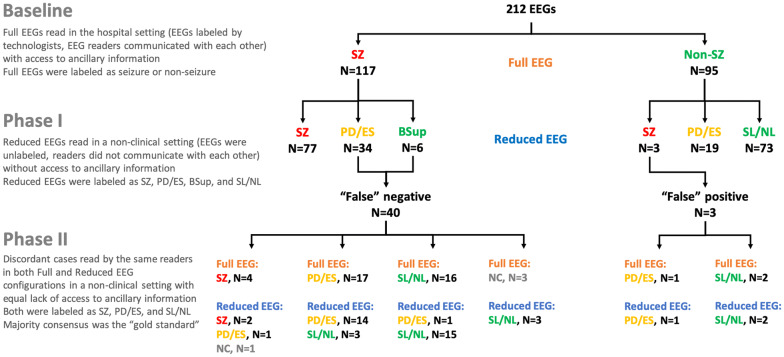
We retrospectively collected 212 adult EEGs recorded at Massachusetts General Hospital and reviewed by two epileptologists with access to clinical, trending, and video information. In Phase I of the study, we re-configured the first 4 h of the EEGs in lateral circumferential montage with ten electrodes and asked new readers to interpret the EEGs without access to any other ancillary information. We compared their rating to the reading of hospital clinicians with access to ancillary information. In Phase II, we measured the accuracy of the same raters reading representative samples of the discordant EEGs in full and reduced configurations presented randomly by comparing their performance to majority consensus as the gold standard.
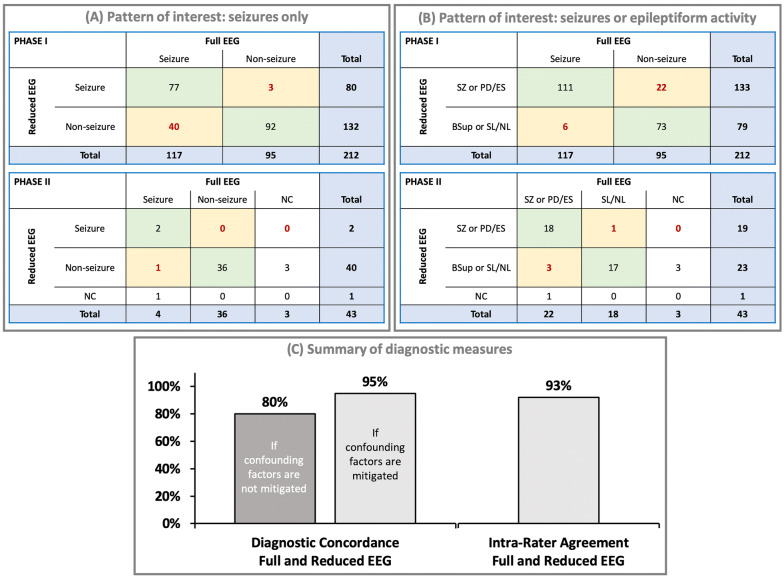
Of the 95 EEGs without seizures in the selected fm-EEG, readers of rm-EEG identified 92 cases (97%) as having no seizure activity. Of 117 EEGs with "seizures" identified in the selected fm-EEG, none of the cases was labeled as normal on rm-EEG. Readers of rm-EEG reported pathological activity in 100% of cases, but labeled them as seizures (N = 77), rhythmic or periodic patterns (N = 24), epileptiform spikes (N = 7), or burst suppression (N = 6). When the same raters read representative epochs of the discordant EEG cases (N = 43) in both fm-EEG and rm-EEG configurations, we found high concordance (95%) and intra-rater agreement (93%) between fm-EEG and rm-EEG diagnoses.
Reduced EEG with ten electrodes in circumferential configuration preserves key features of the traditional EEG system. Discrepancies between rm-EEG and fm-EEG as reported in some of the past studies can be in part due to methodological factors such as choice of gold standard diagnosis, asymmetric access to ancillary clinical information, and inter-rater variability rather than detection failure of rm-EEG as a result of electrode reduction per se.
在重症监护环境中,使用较少电极的脑电图(缩减式脑电图,rm-EEG)可能是传统全导联脑电图(fm-EEG)的一种及时替代方法。然而,过去的研究报告使用 rm-EEG 检测癫痫发作的准确性存在差异。我们假设过去的研究未能区分不同读者对脑电图模式分类的差异与敏感性的差异。本研究的目的是在考虑混杂因素的情况下重新评估 rm-EEG 的诊断价值。
我们回顾性收集了马萨诸塞州综合医院记录的 212 例成人脑电图,并由两名癫痫专家进行审查,他们可以访问临床、趋势和视频信息。在研究的第一阶段,我们重新配置了第一个 4 小时的脑电图,采用 10 个电极的侧环形导联,并要求新读者在不访问任何其他辅助信息的情况下解释脑电图。我们将他们的评分与可以访问辅助信息的医院临床医生的评分进行比较。在第二阶段,我们通过将他们的表现与多数共识作为金标准进行比较,测量相同评分者在全导联和缩减导联配置中阅读具有代表性的、不一致的脑电图样本的准确性。
在所选择的 fm-EEG 中,95 例无癫痫发作的脑电图中,rm-EEG 的读者将 92 例(97%)识别为无癫痫发作活动。在所选 fm-EEG 中标记为“癫痫发作”的 117 例脑电图中,无一例在 rm-EEG 上被标记为正常。rm-EEG 的读者报告了 100%的病例存在病理性活动,但将其标记为癫痫发作(N=77)、节律或周期性模式(N=24)、癫痫样棘波(N=7)或爆发抑制(N=6)。当相同的评分者阅读具有代表性的、不一致的脑电图病例(N=43)的脑电图时,我们发现 fm-EEG 和 rm-EEG 之间的诊断具有高度一致性(95%)和评分者内一致性(93%)。
采用环形配置的 10 个电极的缩减式脑电图保留了传统脑电图系统的关键特征。过去的一些研究报告的 rm-EEG 和 fm-EEG 之间的差异部分可能是由于方法学因素,如金标准诊断的选择、对辅助临床信息的不对称访问以及评分者间的变异性,而不是由于电极减少本身导致 rm-EEG 的检测失败。