Diniz-Silva Fabia, Moriya Henrique T, Alencar Adriano M, Amato Marcelo B P, Carvalho Carlos R R, Ferreira Juliana C
Divisao de Pneumologia, Instituto do Coracao, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, SP, BR, Av. Dr. Enéas de Carvalho Aguiar, 44, 5 andar, bloco 2, sala 1, São Paulo, SP, CEP 05403900, Brazil.
Biomedical Engineering Laboratory, Escola Politécnica da USP, Av. Prof. Luciano Gualberto, trav. 3, 158, Cidade Universitária, São Paulo, SP, CEP 05586-0600, Brazil.
Ann Intensive Care. 2020 Feb 10;10(1):18. doi: 10.1186/s13613-020-0638-0.
Protective mechanical ventilation is recommended for patients with acute respiratory distress syndrome (ARDS), but it usually requires controlled ventilation and sedation. Using neurally adjusted ventilatory assist (NAVA) or pressure support ventilation (PSV) could have additional benefits, including the use of lower sedative doses, improved patient-ventilator interaction and shortened duration of mechanical ventilation. We designed a pilot study to assess the feasibility of keeping tidal volume (V) at protective levels with NAVA and PSV in patients with ARDS.
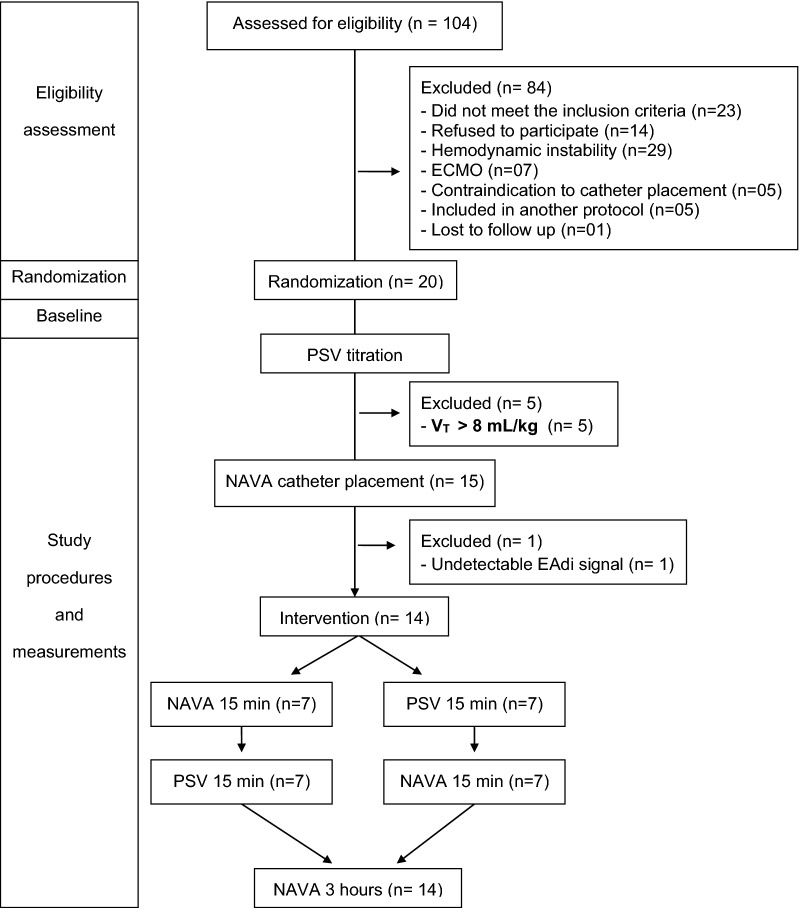
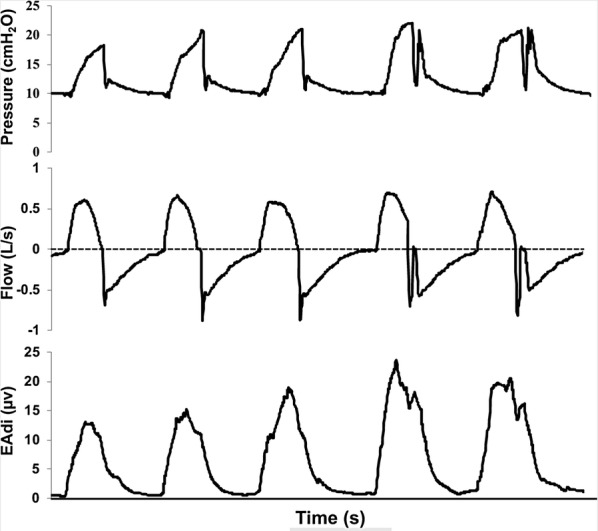
We conducted a prospective randomized crossover trial in five ICUs from a university hospital in Brazil and included patients with ARDS transitioning from controlled ventilation to partial ventilatory support. NAVA and PSV were applied in random order, for 15 min each, followed by 3 h in NAVA. Flow, peak airway pressure (Paw) and electrical activity of the diaphragm (EAdi) were captured from the ventilator, and a software (Matlab, Mathworks, USA), automatically detected inspiratory efforts and calculated respiratory rate (RR) and V. Asynchrony events detection was based on waveform analysis.
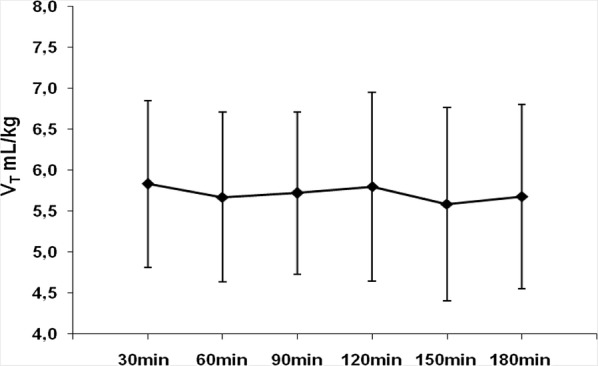
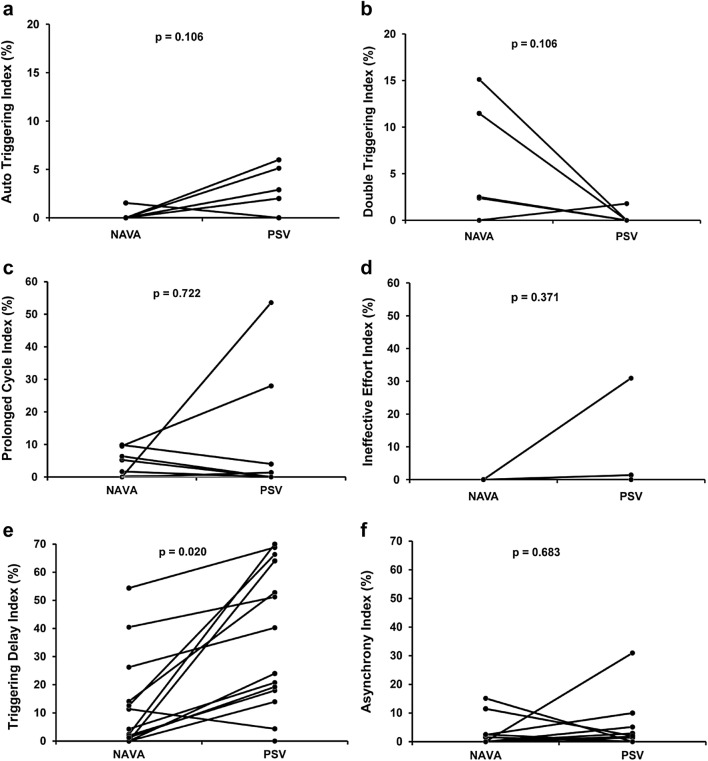
We randomized 20 patients, but the protocol was interrupted for five (25%) patients for whom we were unable to maintain V below 6.5 mL/kg in PSV due to strong inspiratory efforts and for one patient for whom we could not detect EAdi signal. For the 14 patients who completed the protocol, V was 5.8 ± 1.1 mL/kg for NAVA and 5.6 ± 1.0 mL/kg for PSV (p = 0.455) and there were no differences in RR (24 ± 7 for NAVA and 23 ± 7 for PSV, p = 0.661). Paw was greater in NAVA (21 ± 3 cmHO) than in PSV (19 ± 3 cmHO, p = 0.001). Most patients were under continuous sedation during the study. NAVA reduced triggering delay compared to PSV (p = 0.020) and the median asynchrony Index was 0.7% (0-2.7) in PSV and 0% (0-2.2) in NAVA (p = 0.6835).
It was feasible to keep V in protective levels with NAVA and PSV for 75% of the patients. NAVA resulted in similar V, RR and Paw compared to PSV. Our findings suggest that partial ventilatory assistance with NAVA and PSV is feasible as a protective ventilation strategy in selected ARDS patients under continuous sedation. Trial registration ClinicalTrials.gov (NCT01519258). Registered 26 January 2012, https://clinicaltrials.gov/ct2/show/NCT01519258.
对于急性呼吸窘迫综合征(ARDS)患者,推荐采用保护性机械通气,但通常需要控制通气和镇静。使用神经调节通气辅助(NAVA)或压力支持通气(PSV)可能有额外益处,包括使用较低的镇静剂量、改善患者与呼吸机的相互作用以及缩短机械通气时间。我们设计了一项前瞻性研究,以评估在ARDS患者中使用NAVA和PSV将潮气量(V)维持在保护水平的可行性。
我们在巴西一家大学医院的五个重症监护病房进行了一项前瞻性随机交叉试验,纳入从控制通气过渡到部分通气支持的ARDS患者。NAVA和PSV按随机顺序应用,各持续15分钟,随后进行3小时的NAVA通气。从呼吸机获取流量、气道峰压(Paw)和膈肌电活动(EAdi),并使用软件(美国Mathworks公司的Matlab)自动检测吸气努力并计算呼吸频率(RR)和V。基于波形分析检测不同步事件。
我们将20例患者随机分组,但该方案因5例(2 * 5%)患者而中断,这5例患者由于强烈的吸气努力,我们无法在PSV中将V维持在6.5 mL/kg以下,还有1例患者我们无法检测到EAdi信号。对于完成该方案的14例患者,NAVA时V为5.8±1.1 mL/kg,PSV时V为5.6±1.0 mL/kg(p = 0.455),RR无差异(NAVA时为24±7,PSV时为23±7,p = 0.661)。NAVA时的Paw(21±3 cmH₂O)高于PSV时(19±3 cmH₂O,p = 0.001)。在研究期间,大多数患者接受持续镇静。与PSV相比,NAVA减少了触发延迟(p = 0.020),PSV时不同步指数中位数为0.7%(0 - 2.7),NAVA时为0%(0 - 2.2)(p = 0.6835)。
对于75%的患者,使用NAVA和PSV将V维持在保护水平是可行的。与PSV相比,NAVA导致的V、RR和Paw相似。我们的研究结果表明,在持续镇静的特定ARDS患者中,采用NAVA和PSV进行部分通气辅助作为一种保护性通气策略是可行的。试验注册ClinicalTrials.gov(NCT01519258)。于2012年1月26日注册,https://clinicaltrials.gov/ct2/show/NCT01519258 。