Gajdács Márió, Bátori Zoltán, Ábrók Marianna, Lázár Andrea, Burián Katalin
Department of Pharmacodynamics and Biopharmacy, Faculty of Pharmacy, University of Szeged, 6720 Szeged, Eötvös utca 6., Hungary.
Department of Ecology, Faculty of Sciences, University of Szeged, 6726 Szeged, Közép fasor 52., Hungary.
Life (Basel). 2020 Feb 11;10(2):16. doi: 10.3390/life10020016.
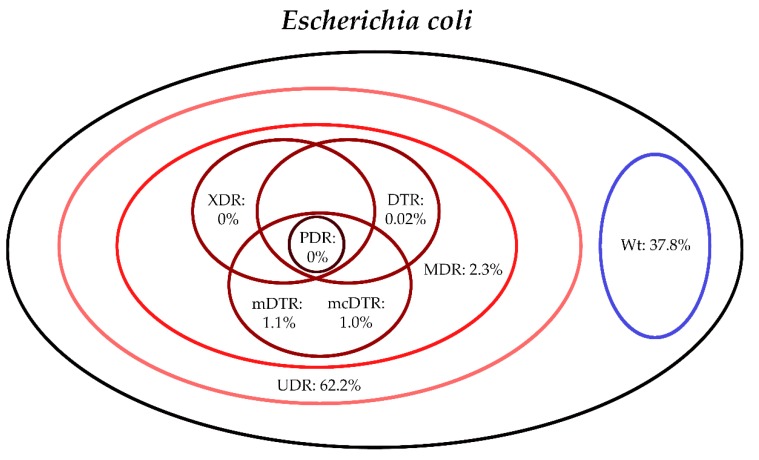
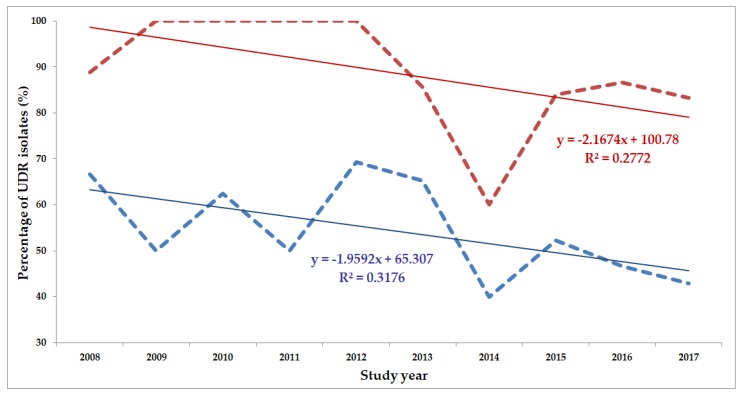
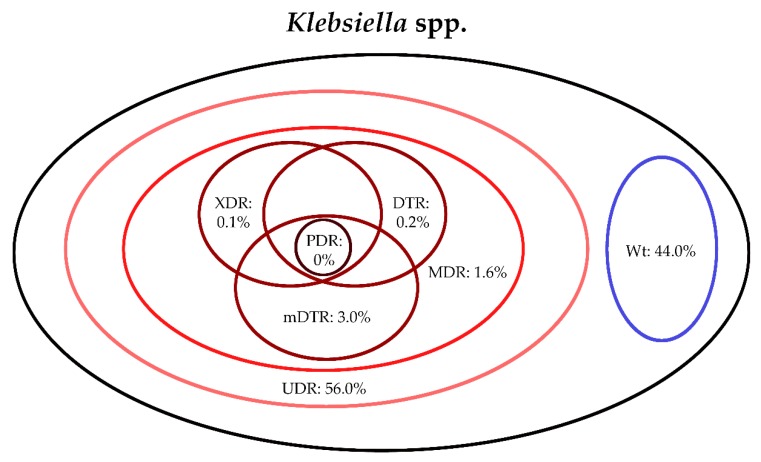
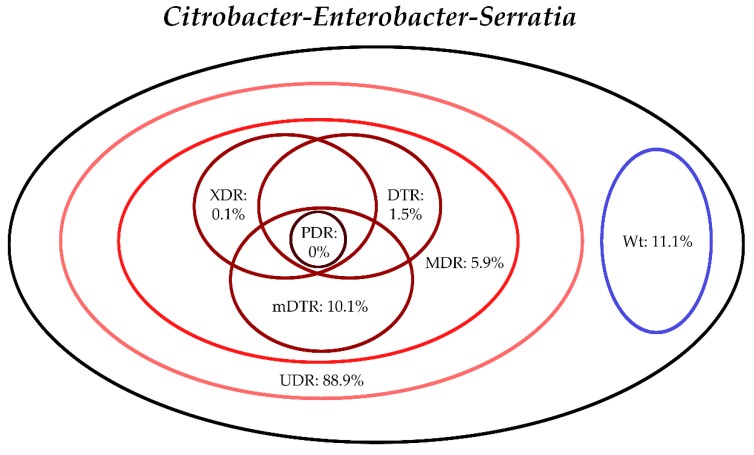
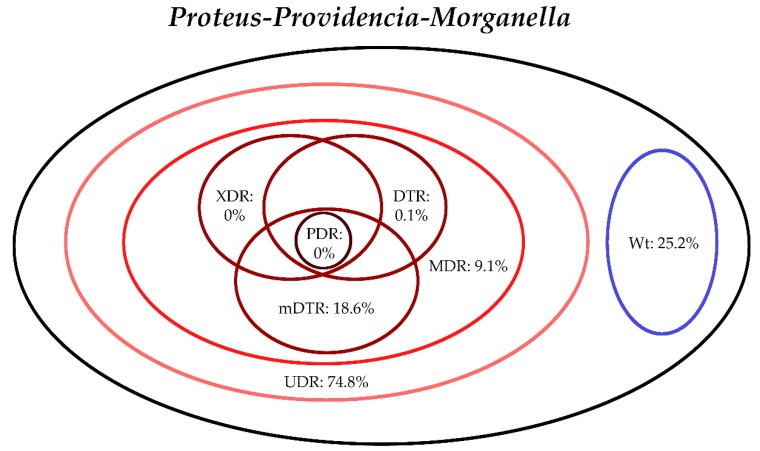
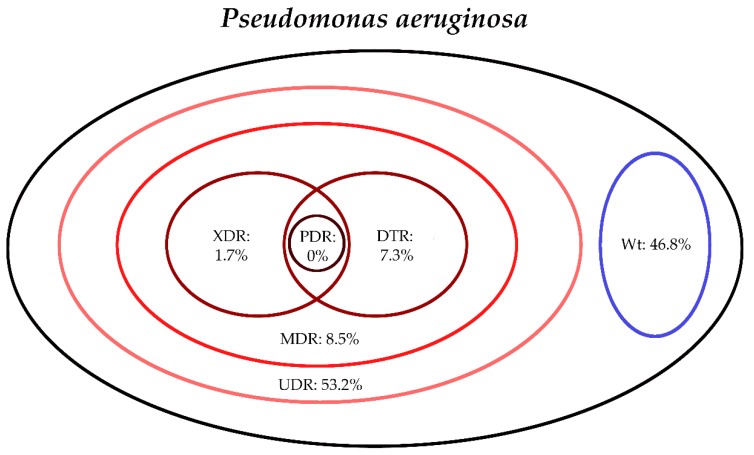
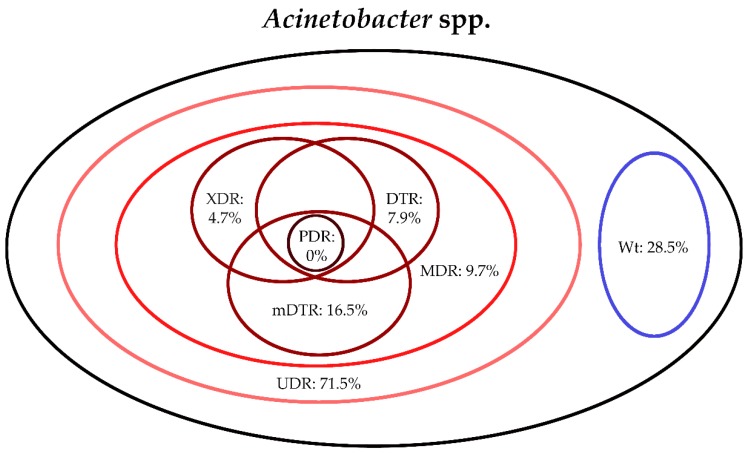
Classical resistance classifications (multidrug resistance [MDR], extensive drug resistance [XDR], pan-drug resistance [PDR]) are very useful for epidemiological purposes, however, they may not correlate well with clinical outcomes, therefore, several novel classification criteria (e.g., usual drug resistance [UDR], difficult-to-treat resistance [DTR]) were introduced for Gram-negative bacteria in recent years. Microbiological and resistance data was collected for urinary tract infections (UTIs) retrospectively, corresponding to the 2008.01.01-2017.12.31. period. Isolates were classified into various resistance categories (wild type/susceptible, UDR, MDR, XDR, DTR and PDR), in addition, two new indicators (modified DTR; mDTR and mcDTR) and a predictive composite score (pMAR) were introduced. Results n = 16,240 (76.8%) outpatient and n = 13,386 (69.3%) inpatient UTI isolates were relevant to our analysis. had the highest level of UDR isolates (88.9%), the group had the highest mDTR levels. MDR levels were highest in spp. (9.7%) and (9.1%). XDR- and DTR-levels were higher in non-fermenters (XDR: 1.7%-4.7%. DTR: 7.3%-7.9%) than in isolates (XDR: 0%-0.1%. DTR: 0.02%-1.5%). Conclusions The introduction of DTR (and its' modifications detailed in this study) to the bedside and in clinical practice will definitely lead to substantial benefits in the assessment of the significance of bacterial resistance in human therapeutics.
经典的耐药性分类(多重耐药 [MDR]、广泛耐药 [XDR]、全耐药 [PDR])对于流行病学目的非常有用,然而,它们可能与临床结果相关性不佳,因此,近年来针对革兰氏阴性菌引入了几种新的分类标准(例如,常见耐药 [UDR]、难治性耐药 [DTR])。回顾性收集了2008年1月1日至2017年12月31日期间尿路感染(UTI)的微生物学和耐药性数据。分离株被分类为各种耐药类别(野生型/敏感、UDR、MDR、XDR、DTR和PDR),此外,还引入了两个新指标(改良DTR;mDTR和mcDTR)和一个预测性综合评分(pMAR)。结果n = 16,240(76.8%)门诊和n = 13,386(69.3%)住院UTI分离株与我们的分析相关。 组的UDR分离株水平最高(88.9%), 组的mDTR水平最高。MDR水平在 菌属(9.7%)和 菌属(9.1%)中最高。非发酵菌的XDR和DTR水平(XDR:1.7% - 4.7%,DTR:7.3% - 7.9%)高于 分离株(XDR:0% - 0.1%,DTR:0.02% - 1.5%)。结论将DTR(以及本研究中详细描述的其修改形式)引入床边和临床实践肯定会在评估人类治疗中细菌耐药性的重要性方面带来实质性益处。