Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Department of Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
J Korean Med Sci. 2020 Feb 17;35(6):e36. doi: 10.3346/jkms.2020.35.e36.
Prophylaxis for hepatitis B virus (HBV) recurrence is essential after liver transplantation (LT) in HBV-associated recipients. We conducted real-world analysis of HBV prophylaxis after LT in the Korean population.
Korean Organ Transplantation Registry (KOTRY) database and additionally collected data (n = 326) were analyzed with special reference to types of HBV prophylaxis.
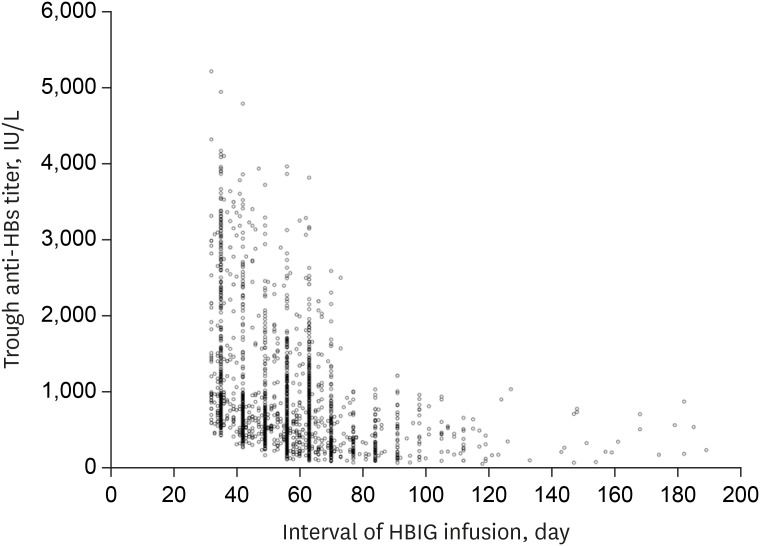
The study cohort comprised 267 cases of living-donor LT and 59 cases of deceased-donor LT. Hepatocellular carcinoma (HCC) was diagnosed in 232 (71.2%) of these subjects. Antiviral agents were used in 255 patients (78.2%) prior to LT. HBV DNA was undetectable in 69 cases (21.2%) and detectable over wide concentrations in the other 257 patients (78.8%) prior to LT. Polymerase chain reaction analysis of the store blood samples detected HBV DNA in all patients, with 159 patients (48.9%) showing concentrations > 100 IU/mL. Post-transplant HBV regimens during the first year included combination therapy in 196 (60.1%), hepatitis B immunoglobulin (HBIG) monotherapy in 121 (37.1%), and antiviral monotherapy in 9 (2.8%). In the second post-transplant year, these regimens had changed to combination therapy in 187 (57.4%), HBIG monotherapy in 112 (34.4%), and antiviral monotherapy in 27 (8.3%). Trough antibody to hepatitis B surface antigen titers > 500 IU/mL and >1,000 IU/mL were observed in 61.7% and 25.2%, respectively. The mean simulative half-life of HBIG was 21.6 ± 4.3 days with a median 17.7 days. Up to 2-year follow-up period, HCC recurrence and HBV recurrence developed in 18 (5.5%) and 6 (1.8%), respectively. HCC recurrence developed in 3 of 6 patients with HBV recurrence.
Combination therapy is the mainstay of HBV prophylaxis protocols in a majority of Korean LT centers, but HBIG was often administered excessively. Individualized optimization of HBIG treatments using SHL is necessary to adjust the HBIG infusion interval.
在乙型肝炎病毒(HBV)相关受者进行肝移植(LT)后,预防 HBV 复发至关重要。我们对韩国人群中 LT 后 HBV 预防进行了真实世界分析。
对韩国器官移植登记处(KOTRY)数据库和额外收集的数据(n=326)进行了分析,特别参考了 HBV 预防的类型。
研究队列包括 267 例活体供者 LT 和 59 例死体供者 LT。232 例(71.2%)患者诊断为肝细胞癌(HCC)。255 例患者在 LT 前使用了抗病毒药物(78.2%)。69 例患者(21.2%)在 LT 前 HBV DNA 不可检测,而其他 257 例患者(78.8%)HBV DNA 浓度广泛可检测。对所有患者的储存血样进行聚合酶链反应分析均检测到 HBV DNA,其中 159 例患者(48.9%)浓度>100 IU/mL。移植后第一年的 HBV 方案包括联合治疗 196 例(60.1%)、乙肝免疫球蛋白(HBIG)单药治疗 121 例(37.1%)和抗病毒单药治疗 9 例(2.8%)。在移植后的第二年,这些方案在 187 例(57.4%)中转变为联合治疗,112 例(34.4%)为 HBIG 单药治疗,27 例(8.3%)为抗病毒单药治疗。观察到抗乙型肝炎表面抗原抗体的血清浓度>500 IU/mL 和>1000 IU/mL 分别为 61.7%和 25.2%。HBIG 的平均模拟半衰期为 21.6±4.3 天,中位数为 17.7 天。在 2 年的随访期间,分别有 18 例(5.5%)和 6 例(1.8%)发生 HCC 复发和 HBV 复发。HBV 复发的 6 例患者中有 3 例发生 HCC 复发。
在大多数韩国 LT 中心,联合治疗是 HBV 预防方案的主要方法,但 HBIG 常被过度使用。使用 SHL 对 HBIG 治疗进行个体化优化以调整 HBIG 输注间隔是必要的。