Montero María Milagro, López Montesinos Inmaculada, Knobel Hernando, Molas Ema, Sorlí Luisa, Siverio-Parés Ana, Prim Nuria, Segura Concepción, Duran-Jordà Xavier, Grau Santiago, Horcajada Juan Pablo
Infectious Diseases Service, Hospital del Mar, Infectious Pathology and Antimicrobials Research Group (IPAR), Institut Hospital del Mar d'Investigacions Mèdiques (IMIM), Universitat Autònoma de Barcelona (UAB), CEXS-Universitat Pompeu Fabra, Spanish Network for Research in Infectious Diseases (REIPI), 08003 Barcelona, Spain.
Microbiology Service, Laboratori de Referència de Catalunya, Hospital del Mar, 08820 Barcelona, Spain.
J Clin Med. 2020 Feb 14;9(2):514. doi: 10.3390/jcm9020514.
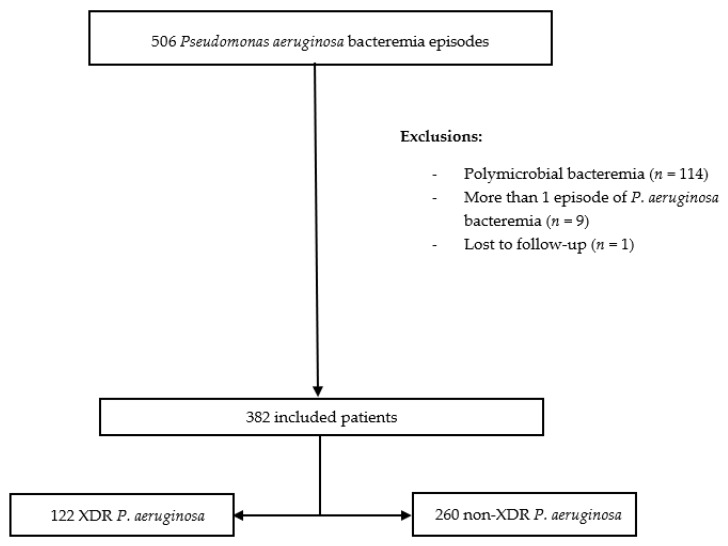
This study aimed to assess the impact of extensively drug-resistant (XDR) phenotype on mortality in bacteremia. A retrospective cohort study was performed in a tertiary hospital from January 2000 to December 2018. All consecutive prospectively recorded bacteremia in adult patients were assessed. In this study, 382 patients were included, of which 122 (31.9%) due to XDR . Independent factors associated with 14-day mortality were as follows: high-risk source of bacteremia (hazard ratio (HR) 3.07, 95% confidence interval (CI), 1.73-5.46), septic shock (HR 1.75, 95% CI, 1.12-2.75), and higher Pitt scores (one-point increments; HR 1.25, 95% CI, 1.12-1.38). Otherwise, the appropriateness of definitive antibiotic therapy was a protective factor (HR 0.39, 95% CI, 0.24-0.62). The same variables were also associated with 30-day mortality. XDR phenotype was not associated with 14- or 30-day mortality. In a subanalysis considering only high-risk source cases, combined antimicrobial therapy was independently associated with 14-day favorable outcome (HR 0.56, 95% CI, 0.33-0.93). In conclusion, XDR phenotype was not associated with poor prognosis in patients with bacteremia in our cohort. However, source of infection, clinical severity, and inappropriate definitive antibiotic therapy were risk factors for mortality. Combined antimicrobial therapy should be considered for high-risk sources.
本研究旨在评估广泛耐药(XDR)表型对菌血症患者死亡率的影响。2000年1月至2018年12月在一家三级医院进行了一项回顾性队列研究。对成年患者所有连续前瞻性记录的菌血症病例进行评估。本研究纳入了382例患者,其中122例(31.9%)为XDR菌血症。与14天死亡率相关的独立因素如下:菌血症高危来源(风险比(HR)3.07,95%置信区间(CI)为1.73 - 5.46)、感染性休克(HR 1.75,95%CI为1.12 - 2.75)以及较高的皮特评分(评分每增加1分;HR 1.25,95%CI为1.12 - 1.38)。此外,确定性抗生素治疗的恰当性是一个保护因素(HR 0.39,95%CI为0.24 - 0.62)。相同的变量也与30天死亡率相关。XDR表型与14天或30天死亡率无关。在仅考虑高危来源病例的亚分析中,联合抗菌治疗与14天良好预后独立相关(HR 0.56,95%CI为0.33 - 0.93)。总之,在我们的队列中,XDR表型与菌血症患者的不良预后无关。然而,感染源、临床严重程度以及不恰当的确定性抗生素治疗是死亡率的危险因素。对于高危来源应考虑联合抗菌治疗。