School of Psychology, University of Leeds, Leeds, England, UK.
BMC Health Serv Res. 2020 Feb 22;20(1):133. doi: 10.1186/s12913-020-4942-z.
Preventing the onset of poor mental health in adolescence is an international public health priority. Universal, whole school preventative approaches are valued for their reach, and anti-stigmatising and resilience building principles. Mindfulness approaches to well-being have the potential to be effective when delivered as a whole school approach for both young people and staff. However, despite growing demand, there is little understanding of possible and optimal ways to implement a mindfulness, whole school approach (M-WSA) to well-being. This study aimed to identify the determinants of early implementation success of a M-WSA. We tested the capacity of the Consolidated Framework for Implementation Research (CFIR), to capture the determinants of the implementation of a mental health intervention in a school setting.
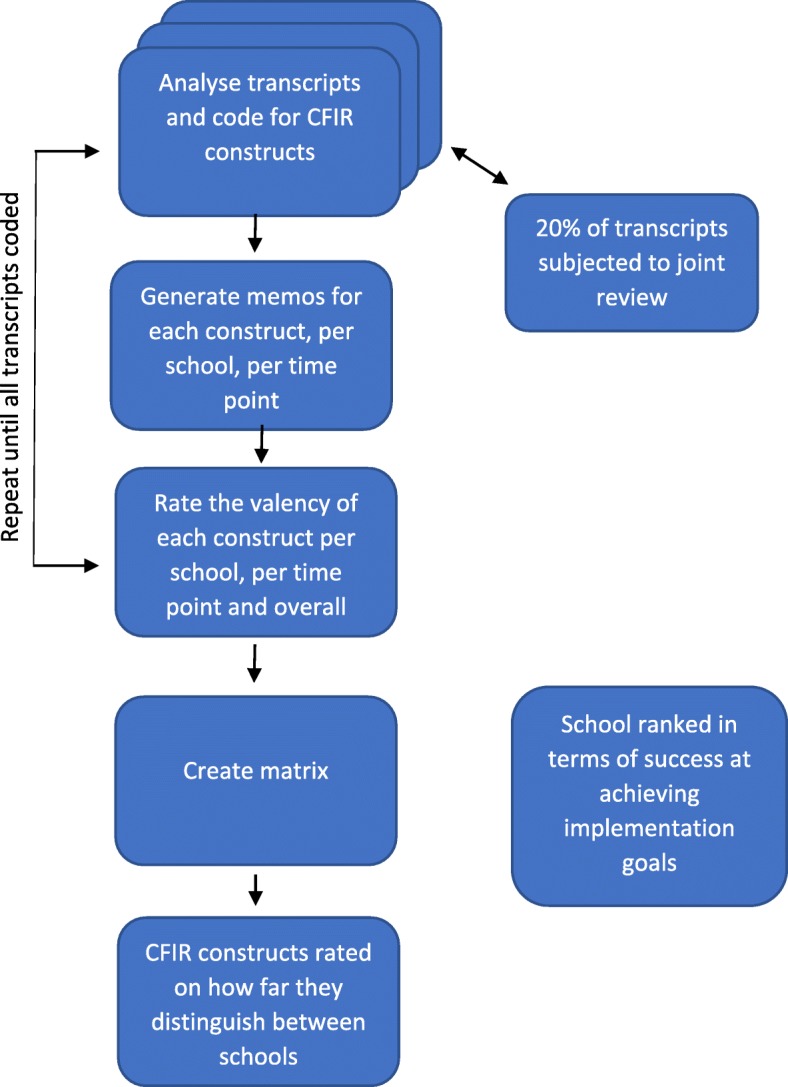
Key members of school staff (n = 15) from five UK secondary schools attempting to implement a M-WSA were interviewed at two-time points, 6 months apart, generating a total of 30 interviews. Interviews explored participants' attitudes, beliefs and experiences around implementing a M-WSA. Interview data were coded as CFIR constructs or other (non CFIR) factors affecting implementation. We also mapped school-reported implementation activity and perceived success over 30 months.
The CFIR captured the implementation activities and challenges well, with 74% of CFIR constructs identifiable in the dataset. Of the 38 CFIR constructs, 11 appeared to distinguish between high and low implementation schools. The most essential construct was school leadership. It strongly distinguished between high and low implementation schools and appeared inter-related with many other distinguishing constructs. Other strongly distinguishing constructs included relative priority, networks and communications, formally appointed implementation leaders, knowledge and beliefs about the intervention, and executing.
Our findings suggest key implementation constructs that schools, commissioners and policy makers should focus on to promote successful early implementation of mental health programs. School leadership is a key construct to target at the outset. The CFIR appears useful for assessing the implementation of mental health programs in UK secondary schools.
预防青少年心理健康问题的发生是国际公共卫生的优先事项。普及性的、面向全体学生的预防措施因其覆盖面广、具有反污名化和培养韧性的原则而受到重视。正念方法在促进幸福感方面具有潜力,如果作为面向学生和教职员工的整体学校方法来实施,可能会非常有效。然而,尽管需求不断增长,但对于实施正念整体学校方法(M-WSA)以促进幸福感的可能和最佳方式,人们知之甚少。本研究旨在确定 M-WSA 早期实施成功的决定因素。我们测试了实施研究整合框架(CFIR)的能力,以捕捉学校环境中实施心理健康干预的决定因素。
来自英国五所中学的学校工作人员(n=15)的核心成员在两次时间点进行了访谈,时间间隔为 6 个月,共进行了 30 次访谈。访谈探讨了参与者对实施 M-WSA 的态度、信念和经验。访谈数据被编码为 CFIR 结构或影响实施的其他(非 CFIR)因素。我们还绘制了 30 个月内学校报告的实施活动和感知成功情况。
CFIR 很好地捕捉了实施活动和挑战,数据集中可识别出 74%的 CFIR 结构。在 38 个 CFIR 结构中,有 11 个结构似乎区分了高实施和低实施的学校。最关键的结构是学校领导。它强烈地区分了高实施和低实施的学校,并与许多其他具有区分力的结构相互关联。其他具有强烈区分力的结构包括相对优先级、网络和沟通、正式任命的实施领导者、对干预措施的知识和信念以及执行力。
我们的研究结果表明,学校、委托人和政策制定者应该关注关键的实施结构,以促进心理健康计划的早期成功实施。学校领导是一开始的关键目标。CFIR 似乎可用于评估英国中学心理健康计划的实施情况。