Rabbat Mark, Leipsic Jonathon, Bax Jeroen, Kauh Brian, Verma Rina, Doukas Demetrios, Allen Sorcha, Pontone Gianluca, Wilber David, Mathew Verghese, Rogers Campbell, Lopez John
Division of Cardiology, Loyola University Medical Center, Maywood, IL 60153, USA.
Department of Radiology, St. Paul's Hospital and the University of British Columbia, Vancouver, BC V6T 1Z4, Canada.
J Clin Med. 2020 Feb 24;9(2):604. doi: 10.3390/jcm9020604.
In the United States, the real-world feasibility and outcome of using fractional flow reserve from coronary computed tomography angiography (FFR) is unknown. We sought to determine whether a strategy that combined coronary computed tomography angiography (CTA) and FFR could safely reduce the need for invasive coronary angiography (ICA), as compared to coronary CTA alone.
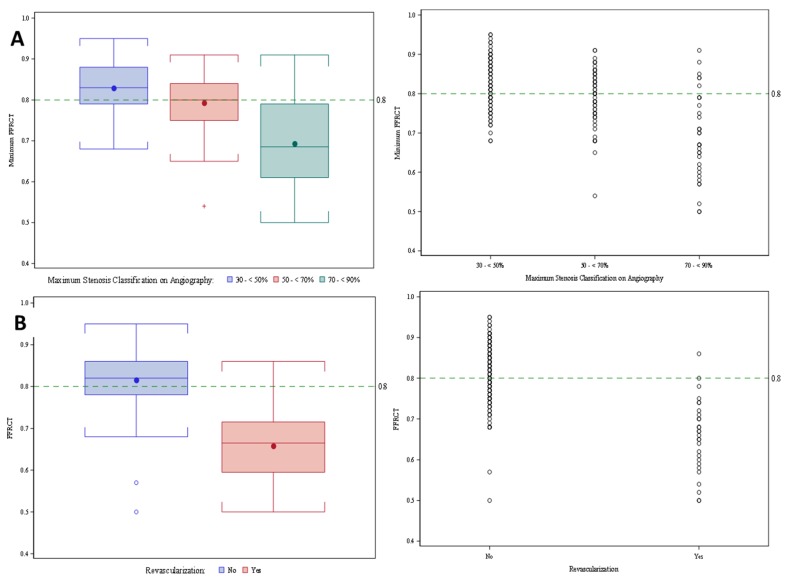
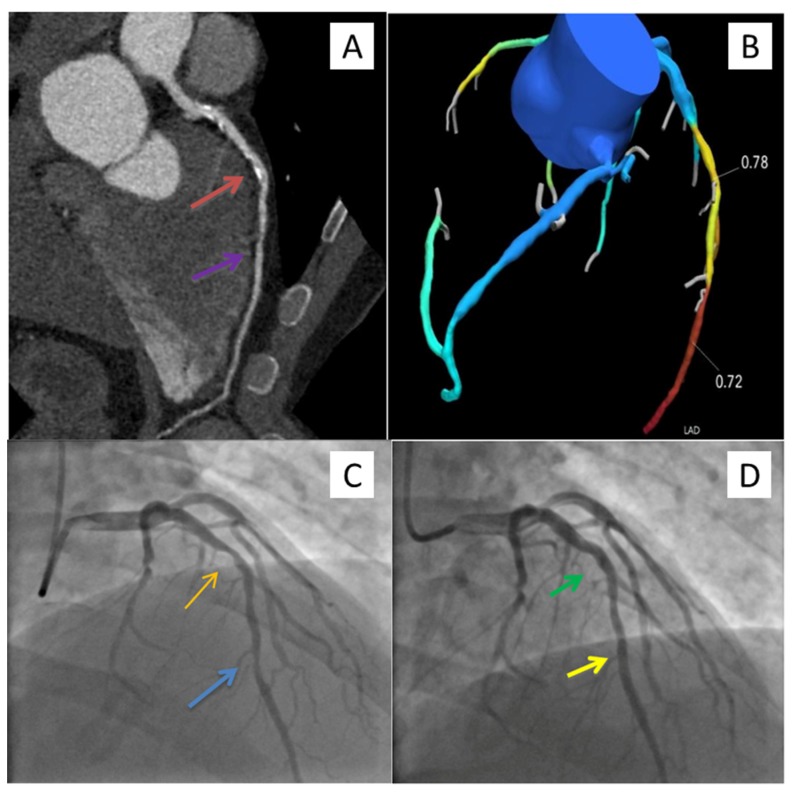
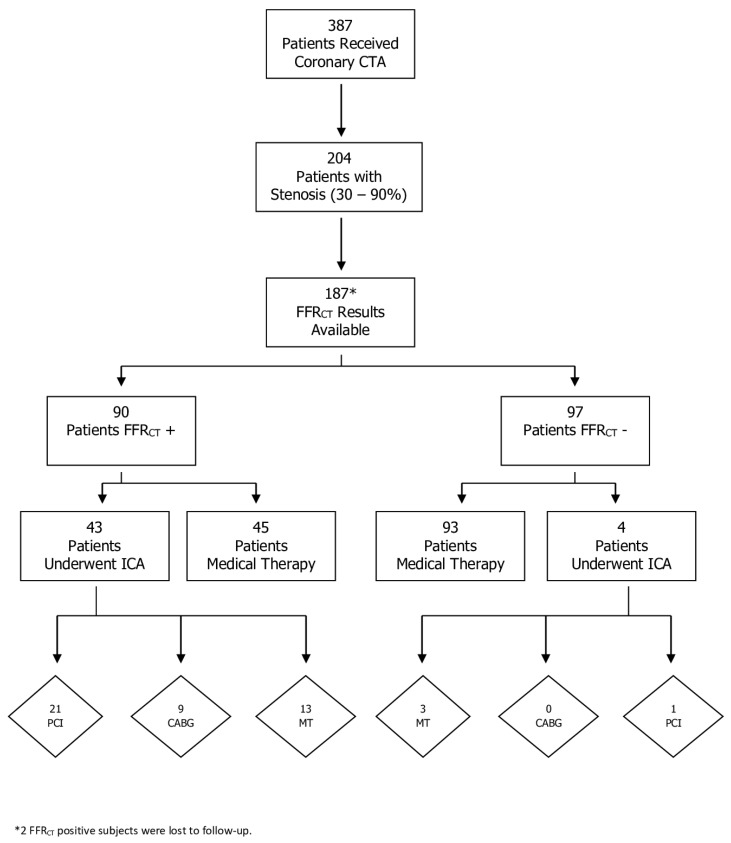
The study included 387 consecutive patients with suspected CAD referred for coronary CTA with selective FFR and 44 control patients who underwent CTA alone. Lesions with 30-90% diameter stenoses were considered of indeterminate hemodynamic significance and underwent FFR. Nadir FFR ≤ 0.80 was positive. The rate of patients having ICA, revascularization and major adverse cardiac events were recorded.
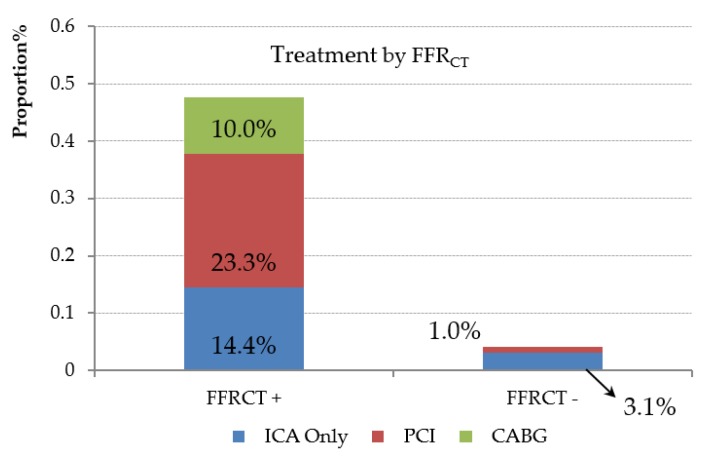
Using coronary CTA and selective FFR, 121 patients (32%) had at least one vessel with ≥50% diameter stenosis; 67/121 (55%) patients had at least one vessel with FFR ≤ 0.80; 55/121 (45%) underwent ICA; and 34 were revascularized. The proportion of ICA patients undergoing revascularization was 62% (34 of 55). The number of patients with vessels with 30-50% diameter of stenosis was 90 (23%); 28/90 (31%) patients had at least one vessel with FFR ≤ 0.80; 8/90 (9%) underwent ICA; and five were revascularized. In our institutional practice, compared to coronary CTA alone, coronary CTA with selective FFR reduced the rates of ICA (45% vs. 80%) for those with obstructive CAD. Using coronary CTA with selective FFR, no major adverse cardiac events occurred over a mean follow-up of 440 days.
FFR safely deferred ICA in patients with CAD of indeterminate hemodynamic significance. A high proportion of those who underwent ICA were revascularized.
在美国,利用冠状动脉计算机断层扫描血管造影(CTA)的血流储备分数(FFR)在现实世界中的可行性和结果尚不清楚。我们试图确定与单独使用冠状动脉CTA相比,联合冠状动脉CTA和FFR的策略是否能安全地减少有创冠状动脉造影(ICA)的需求。
该研究纳入了387例因疑似冠心病而接受冠状动脉CTA检查并选择性进行FFR的连续患者,以及44例仅接受CTA检查的对照患者。直径狭窄30%-90%的病变被认为血流动力学意义不确定,并进行FFR检查。最低FFR≤0.80为阳性。记录进行ICA、血运重建和主要不良心脏事件的患者比例。
使用冠状动脉CTA和选择性FFR,121例患者(32%)至少有一支血管直径狭窄≥50%;67/121例(55%)患者至少有一支血管FFR≤0.80;55/121例(45%)接受了ICA;34例进行了血运重建。接受ICA的患者中进行血运重建的比例为62%(55例中的34例)。直径狭窄30%-50%的血管患者有90例(23%);28/90例(31%)患者至少有一支血管FFR≤0.80;8/90例(9%)接受了ICA;5例进行了血运重建。在我们的机构实践中,与单独使用冠状动脉CTA相比,联合选择性FFR的冠状动脉CTA降低了阻塞性冠心病患者的ICA发生率(45%对80%)。使用联合选择性FFR的冠状动脉CTA,在平均440天的随访期间未发生主要不良心脏事件。
FFR安全地推迟了血流动力学意义不确定的冠心病患者的ICA检查。接受ICA检查的患者中有很大比例进行了血运重建。