Department of Anaesthesia, University Hospitals Morecambe Bay Trust, Royal Lancaster Infirmary, Lancaster, UK.
International Commission for Mountain Emergency Medicine (ICAR MEDCOM), Zermatt, Switzerland.
Scand J Trauma Resusc Emerg Med. 2020 Feb 26;28(1):14. doi: 10.1186/s13049-019-0685-4.
Autoresuscitation describes the return of spontaneous circulation after termination of resuscitation (TOR) following cardiac arrest (CA). We aimed to identify phenomena that may lead to autoresuscitation and to provide guidance to reduce the likelihood of it occurring.
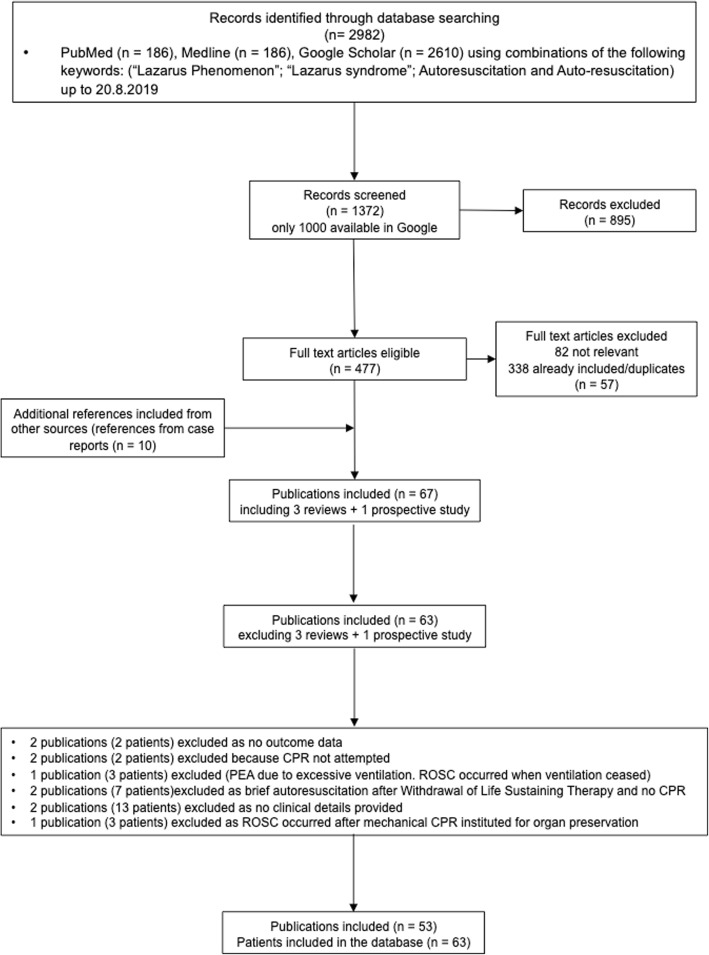
We conducted a literature search (Google Scholar, MEDLINE, PubMed) and a scoping review according to PRISMA-ScR guidelines of autoresuscitation cases where patients undergoing CPR recovered circulation spontaneously after TOR with the following criteria: 1) CA from any cause; 2) CPR for any length of time; 3) A point was reached when it was felt that the patient had died; 4) Staff declared the patient dead and stood back. No further interventions took place; 5) Later, vital signs were observed. 6) Vital signs were sustained for more than a few seconds, such that staff had to resume active care.
Sixty-five patients with ROSC after TOR were identified in 53 articles (1982-2018), 18 (28%) made a full recovery.
Almost a third made a full recovery after autoresuscitation. The following reasons for and recommendations to avoid autoresuscitation can be proposed: 1) In asystole with no reversible causes, resuscitation efforts should be continued for at least 20 min; 2) CPR should not be abandoned immediately after unsuccessful defibrillation, as transient asystole can occur after defibrillation; 3) Excessive ventilation during CPR may cause hyperinflation and should be avoided; 4) In refractory CA, resuscitation should not be terminated in the presence of any potentially-treatable cardiac rhythm; 5) After TOR, the casualty should be observed continuously and ECG monitored for at least 10 min.
自主复苏是指心脏骤停(CA)后心肺复苏(CPR)停止后自发循环恢复。我们旨在确定可能导致自主复苏的现象,并提供指导以降低其发生的可能性。
我们根据 PRISMA-ScR 指南进行了文献检索(Google Scholar、MEDLINE、PubMed)和范围综述,纳入了自主复苏病例,这些病例是指患者在 CPR 停止后 TOR 期间自发恢复循环,符合以下标准:1)任何原因引起的 CA;2)CPR 持续任意时长;3)达到一种认为患者已经死亡的状态;4)医护人员宣布患者死亡并退后;5)不再进行进一步干预;6)随后观察到生命体征。7)生命体征持续超过几秒钟,以至于医护人员必须恢复积极的护理。
在 53 篇文章(1982-2018 年)中确定了 65 例 TOR 后 ROSC 患者,其中 18 例(28%)完全恢复。
近三分之一的患者在自主复苏后完全恢复。可以提出以下避免自主复苏的原因和建议:1)无可逆原因的停搏,CPR 应至少持续 20 分钟;2)除颤失败后不应立即放弃 CPR,因为除颤后可能出现短暂停搏;3)CPR 期间过度通气可能导致过度充气,应避免;4)在难治性 CA 中,在存在任何潜在可治疗的心律时不应终止复苏;5)TOR 后,应连续观察伤员并至少监测 10 分钟心电图。