Shehata Mohamed, Shalaby Ahmed, Switala Andrew E, El-Baz Maryam, Ghazal Mohammed, Fraiwan Luay, Khalil Ashraf, El-Ghar Mohamed Abou, Badawy Mohamed, Bakr Ashraf M, Dwyer Amy, Elmaghraby Adel, Giridharan Guruprasad, Keynton Robert, El-Baz Ayman
BioImaging Lab, Department of Bioengineering, University of Louisville, Louisville, KY, 40208, USA.
Electrical and Computer Engineering Department, Abu Dhabi University, Abu Dhabi, 59911, UAE.
Med Phys. 2020 Jun;47(6):2427-2440. doi: 10.1002/mp.14109. Epub 2020 Apr 3.
Early assessment of renal allograft function post-transplantation is crucial to minimize and control allograft rejection. Biopsy - the gold standard - is used only as a last resort due to its invasiveness, high cost, adverse events (e.g., bleeding, infection, etc.), and the time for reporting. To overcome these limitations, a renal computer-assisted diagnostic (Renal-CAD) system was developed to assess kidney transplant function.
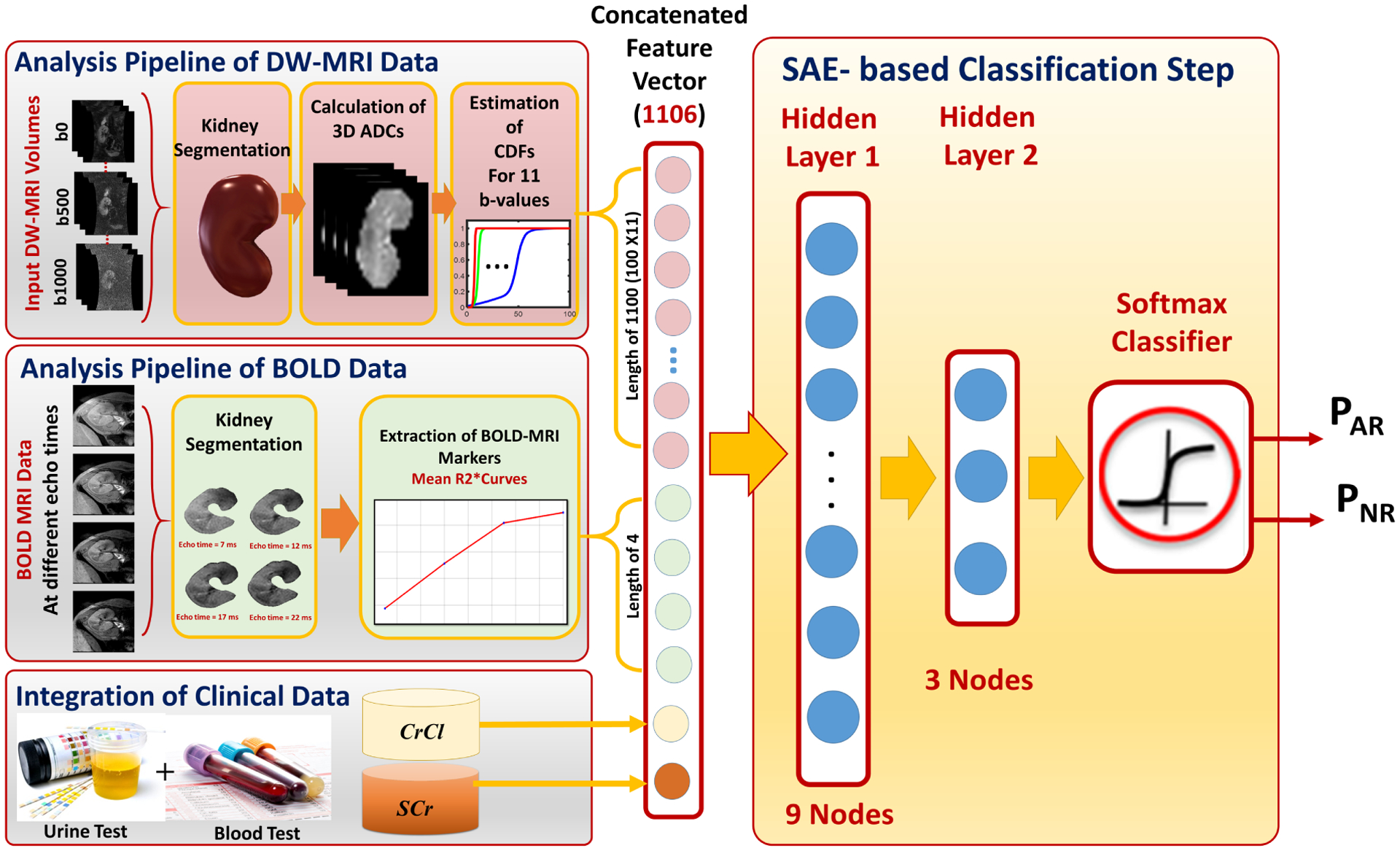
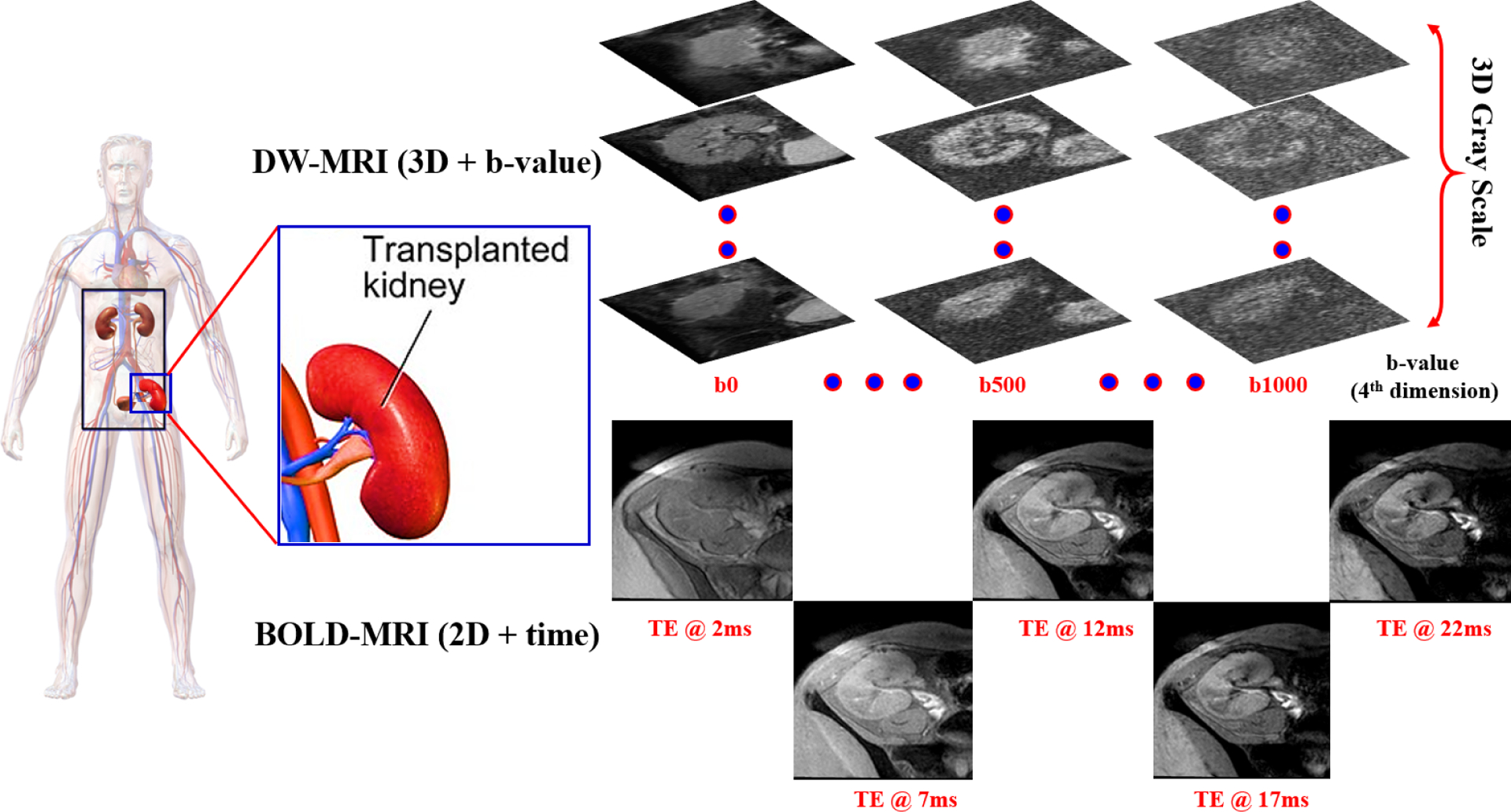
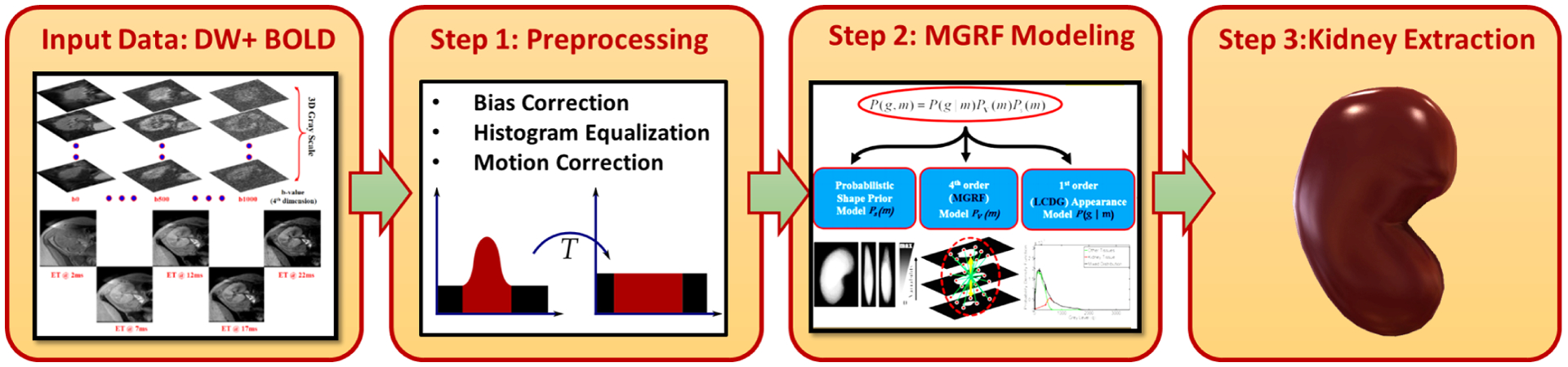
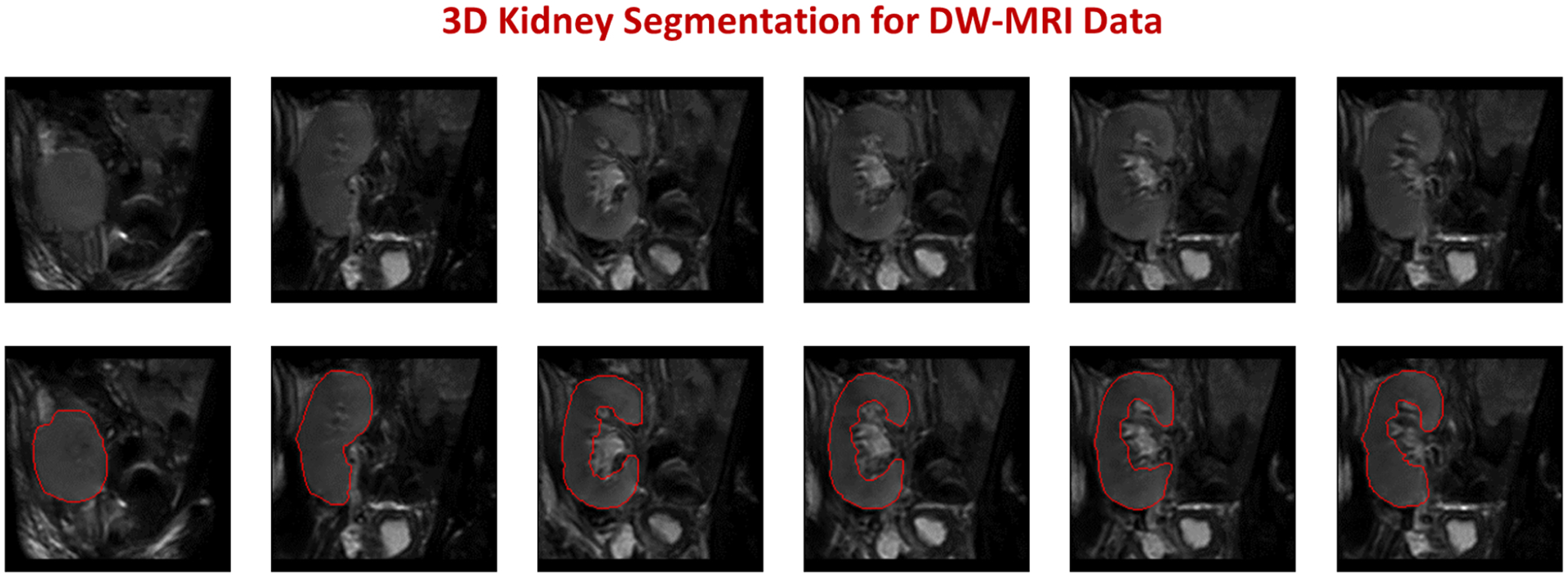
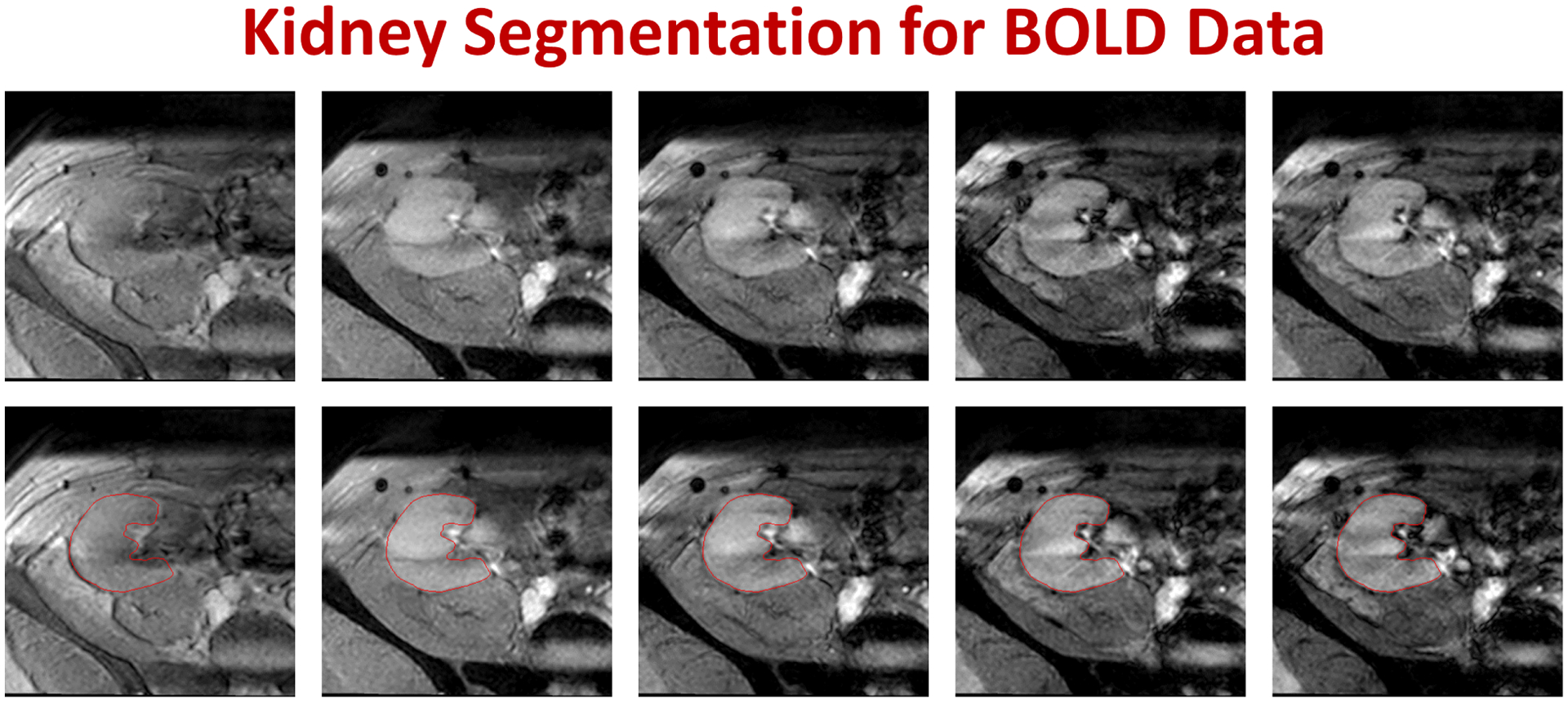
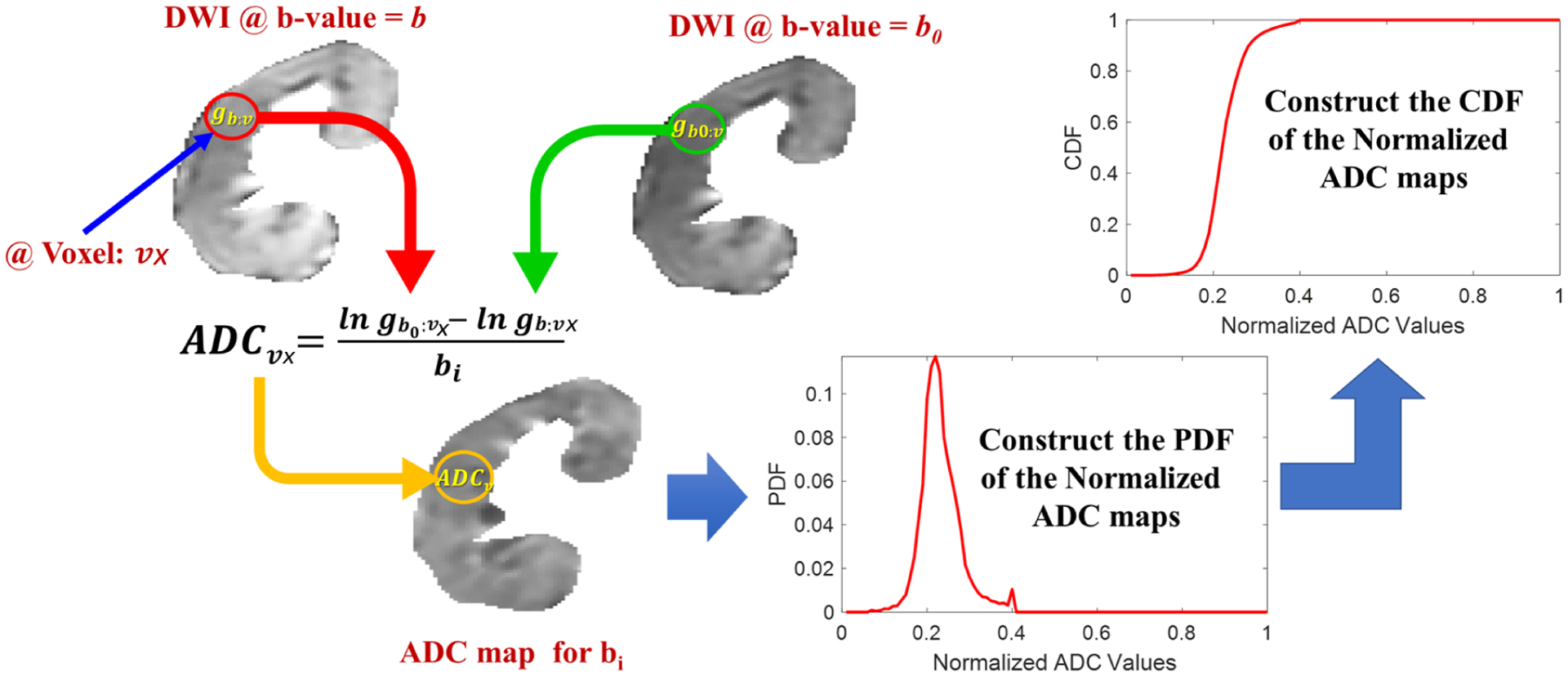
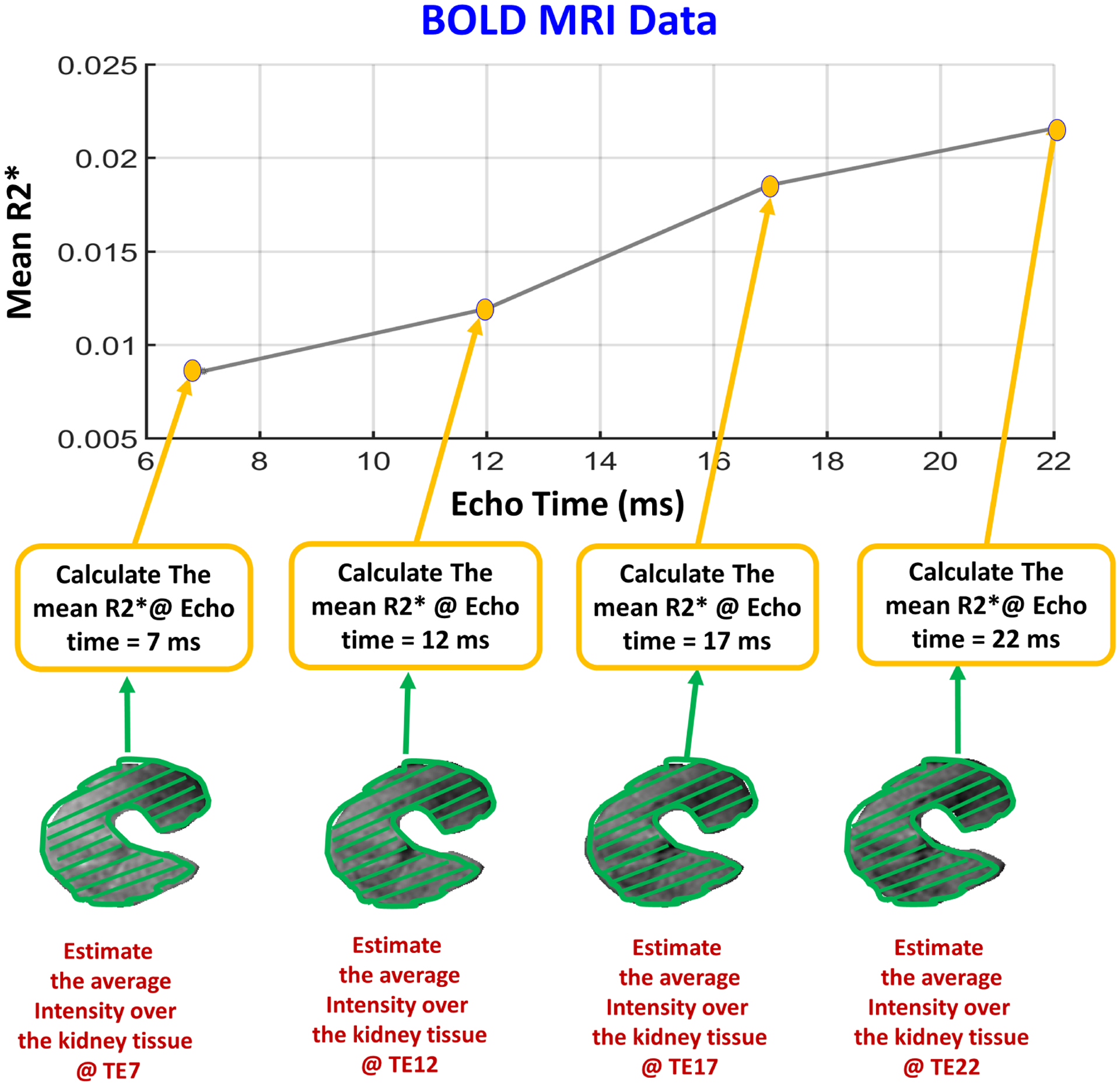
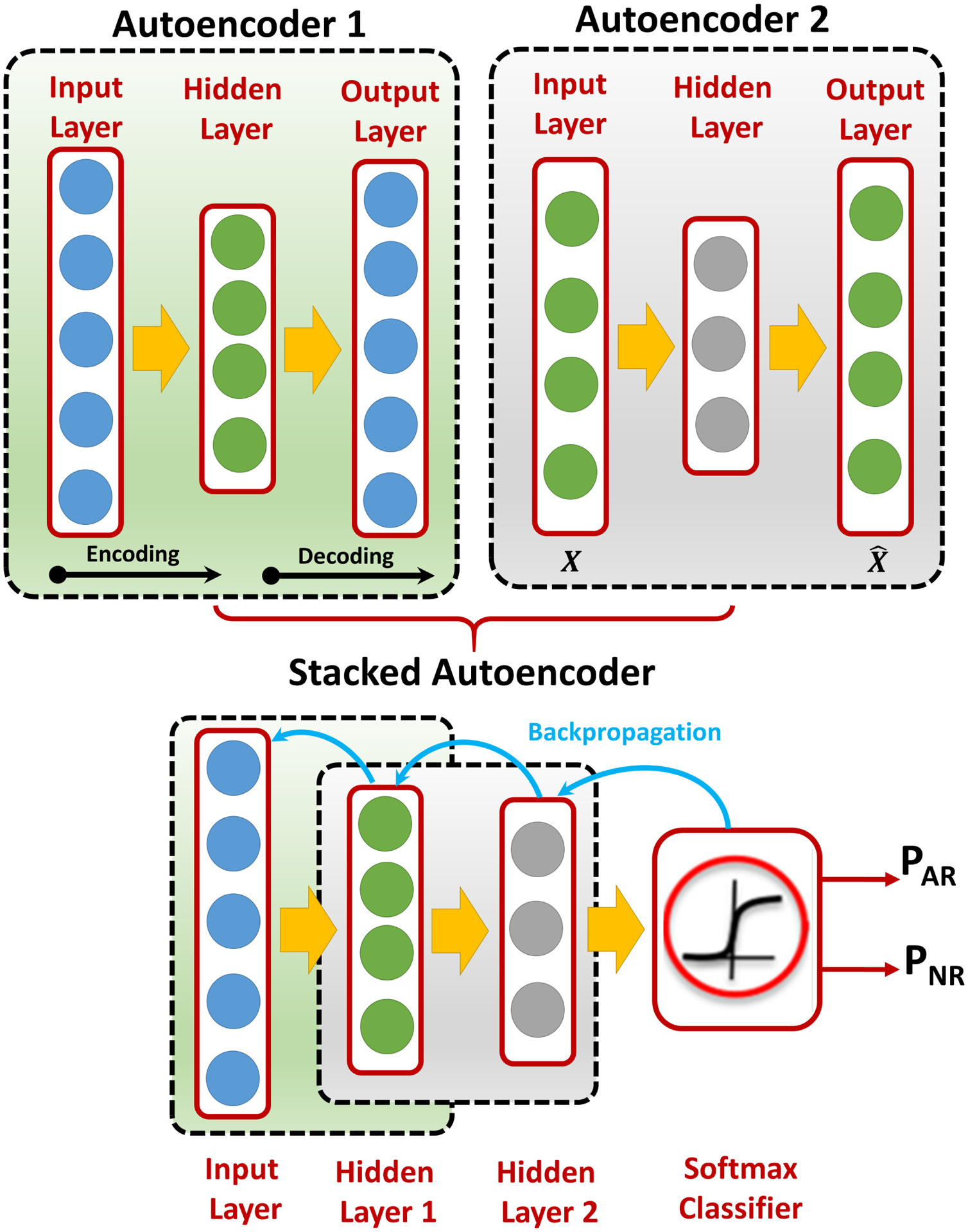
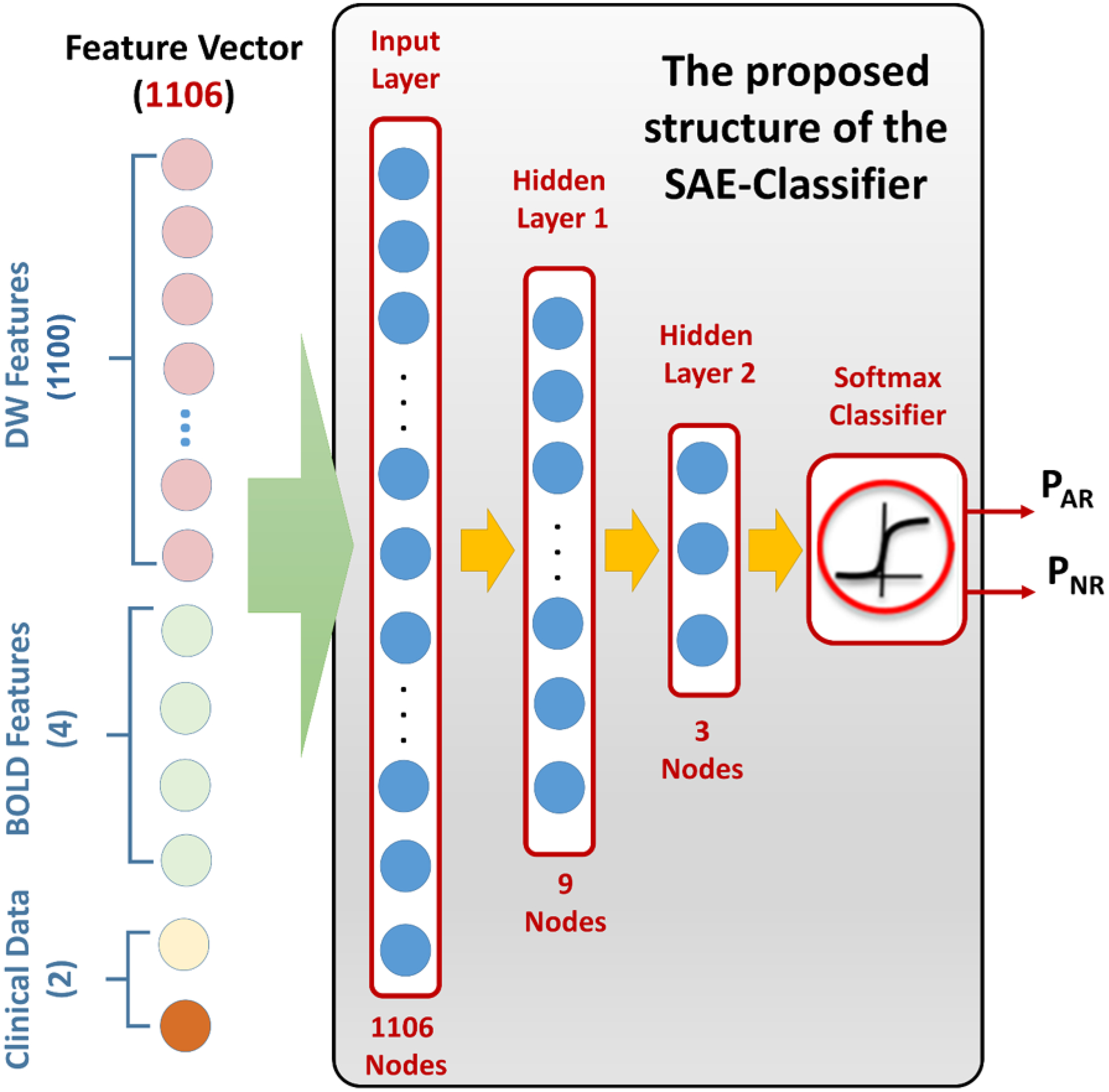
The developed Renal-CAD system integrates data collected from two image-based sources and two clinical-based sources to assess renal transplant function. The imaging sources were the apparent diffusion coefficients (ADCs) extracted from 47 diffusion-weighted magnetic resonance imaging (DW-MRI) scans at 11 different b-values (b0, b50, b100, ..., b1000 s/mm ), and the transverse relaxation rate (R2*) extracted from 30 blood oxygen level-dependent MRI (BOLD-MRI) scans at 5 different echo times (TEs = 2, 7, 12, 17, and 22 ms). Serum creatinine (SCr) and creatinine clearance (CrCl) were the clinical sources for kidney function evaluation. The Renal-CAD system initially performed kidney segmentation using the level-set method, followed by estimation of the ADCs from DW-MRIs and the R2* from BOLD-MRIs. ADCs and R2* estimates from 30 subjects that have both types of scans were integrated with their associated SCr and CrCl. The integrated biomarkers were then used as our discriminatory features to train and test a deep learning-based classifier, namely stacked autoencoders (SAEs) to differentiate non-rejection (NR) from acute rejection (AR) renal transplants.
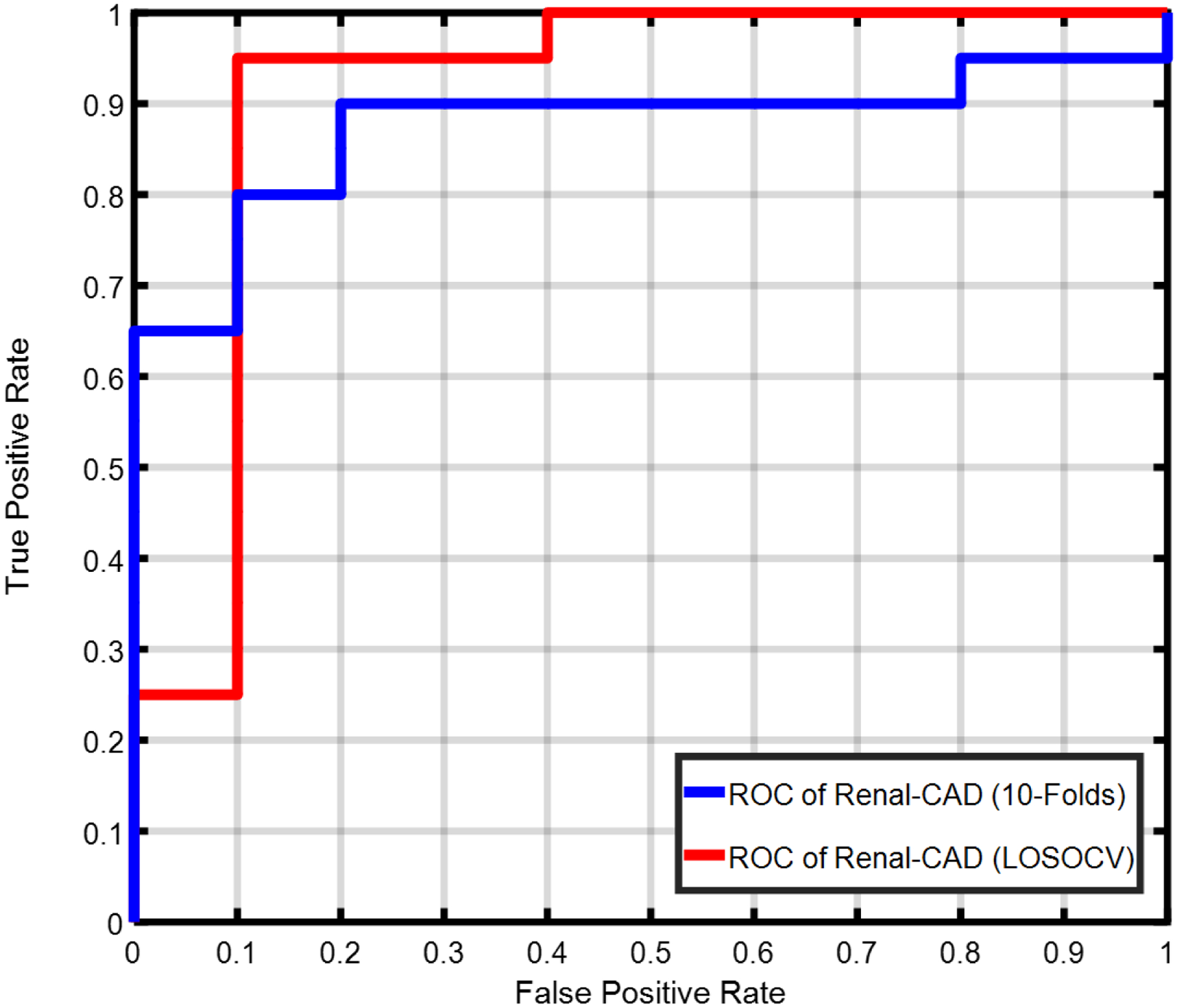
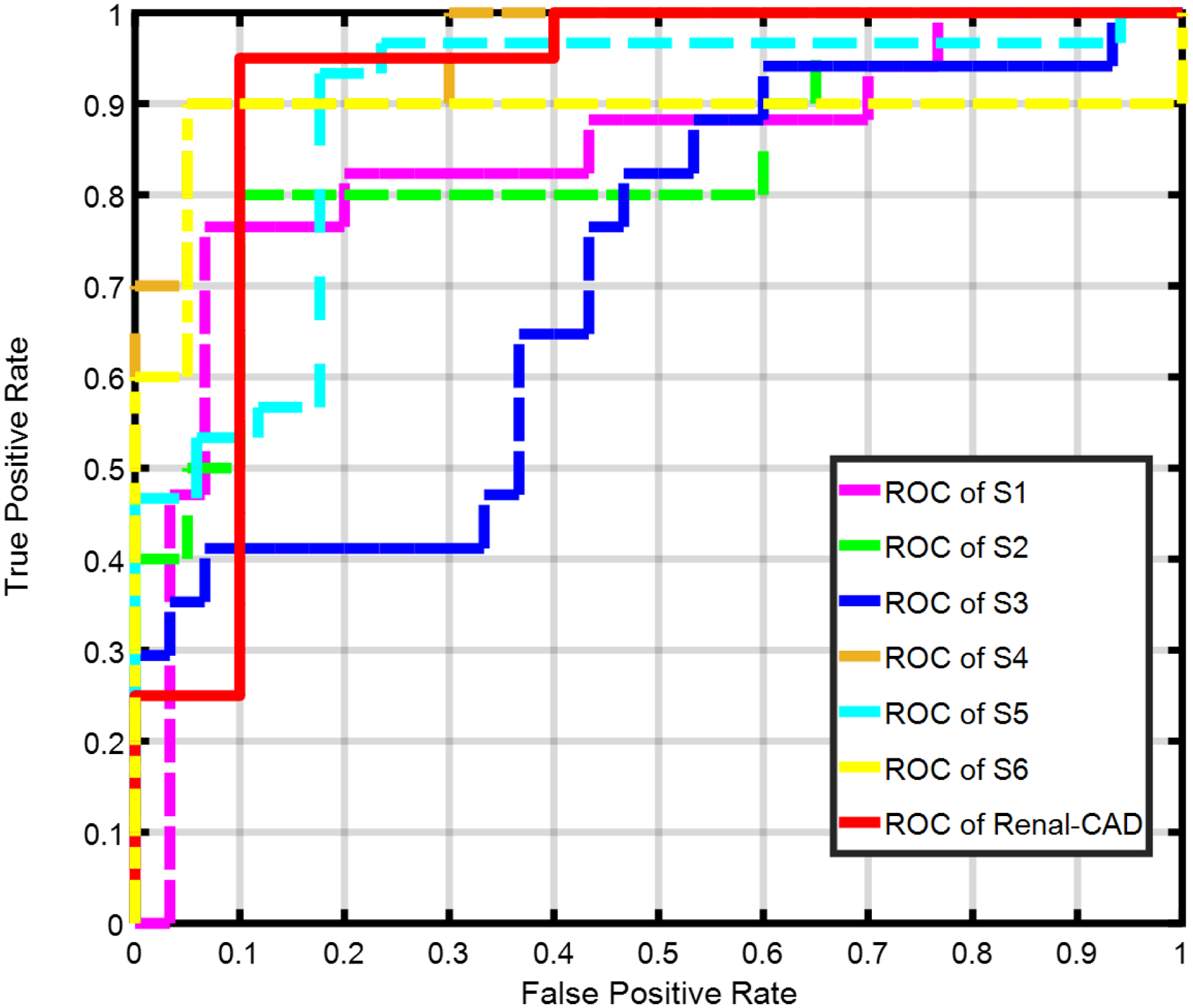
Using a leave-one-subject-out cross-validation approach along with SAEs, the Renal-CAD system demonstrated 93.3% accuracy, 90.0% sensitivity, and 95.0% specificity in differentiating AR from NR. Robustness of the Renal-CAD system was also confirmed by the area under the curve value of 0.92. Using a stratified tenfold cross-validation approach, the Renal-CAD system demonstrated its reproducibility and robustness by a diagnostic accuracy of 86.7%, sensitivity of 80.0%, specificity of 90.0%, and AUC of 0.88.
The obtained results demonstrate the feasibility and efficacy of accurate, noninvasive identification of AR at an early stage using the Renal-CAD system.
肾移植术后早期评估移植肾功能对于最小化和控制移植肾排斥反应至关重要。活检——金标准——由于其侵入性、高成本、不良事件(如出血、感染等)以及报告所需时间,仅作为最后手段使用。为克服这些局限性,开发了一种肾计算机辅助诊断(Renal-CAD)系统来评估肾移植功能。
所开发的Renal-CAD系统整合了从两个基于图像的来源和两个基于临床的来源收集的数据,以评估肾移植功能。成像来源是从11个不同b值(b0、b50、b100、...、b1000 s/mm²)的47次扩散加权磁共振成像(DW-MRI)扫描中提取的表观扩散系数(ADC),以及从5个不同回波时间(TE = 2、7、12、17和22 ms)的30次血氧水平依赖性功能磁共振成像(BOLD-MRI)扫描中提取的横向弛豫率(R2*)。血清肌酐(SCr)和肌酐清除率(CrCl)是评估肾功能的临床来源。Renal-CAD系统最初使用水平集方法进行肾脏分割,随后从DW-MRI估计ADC,从BOLD-MRI估计R2*。将30名同时进行了两种扫描的受试者的ADC和R2*估计值与其相关的SCr和CrCl进行整合。然后将整合后的生物标志物用作我们的鉴别特征,以训练和测试基于深度学习的分类器,即堆叠自编码器(SAE),以区分非排斥(NR)和急性排斥(AR)肾移植。
使用留一法交叉验证方法结合SAE,Renal-CAD系统在区分AR和NR方面表现出93.3%的准确率、90.0%的灵敏度和95.0%的特异性。曲线下面积值为0.92也证实了Renal-CAD系统的稳健性。使用分层十折交叉验证方法,Renal-CAD系统通过86.7%的诊断准确率、80.0%的灵敏度、90.0%的特异性和0.88的AUC证明了其可重复性和稳健性。
所得结果证明了使用Renal-CAD系统在早期准确、无创识别AR的可行性和有效性。