Curcean Andra Diana, Rusu Georgeta Mihaela, Dudea Sorin Marian
Radiology Department, Academic Emergency County Hospital, Cluj-Napoca, Romania.
Radiology Department, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania.
Med Pharm Rep. 2020 Jan;93(1):39-46. doi: 10.15386/mpr-1273. Epub 2020 Jan 31.
Information in ultrasonography about reference values of nerves, particularly of those located in the neck is limited. The aim of the study is to demonstrate the feasibility of direct visualization of the vagus, hypoglossal and greater auricular nerves, testing the method on healthy volunteers and estimate the reference values for two perpendicular diameters and cross-sectional area (CSA).
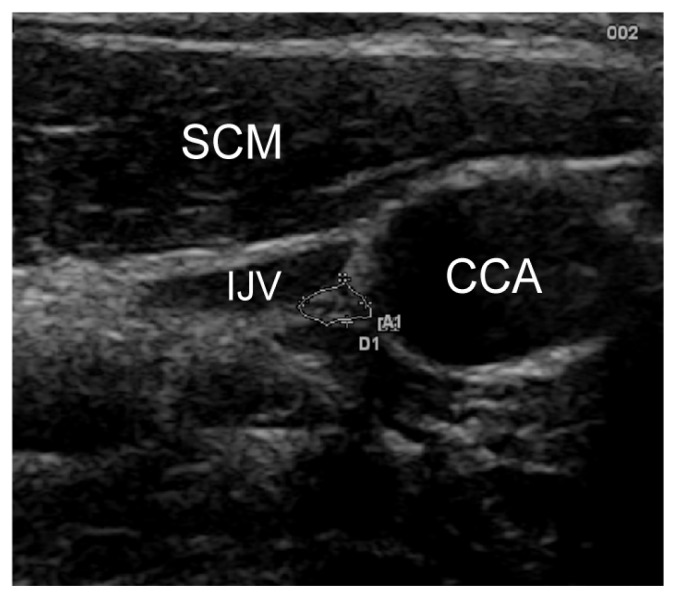
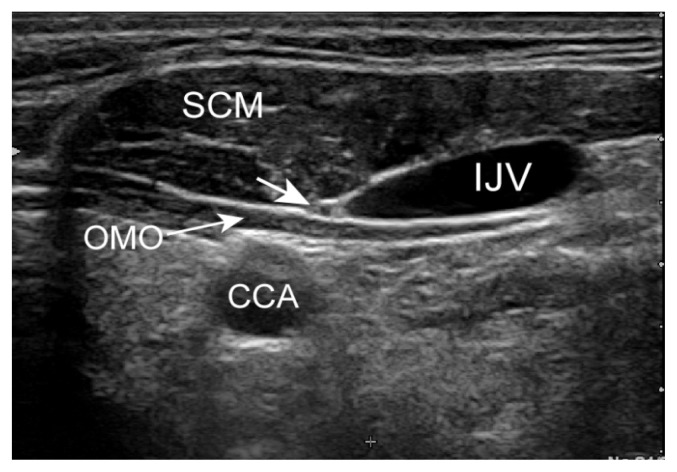
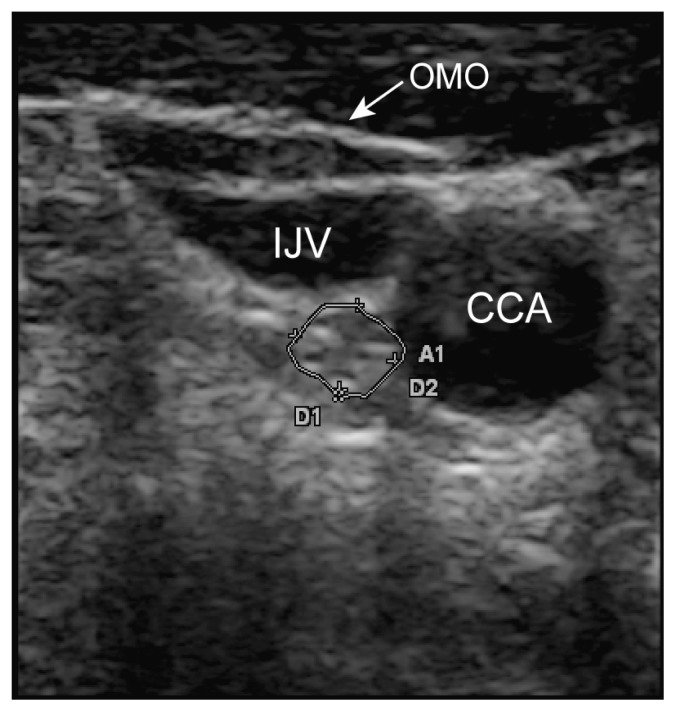
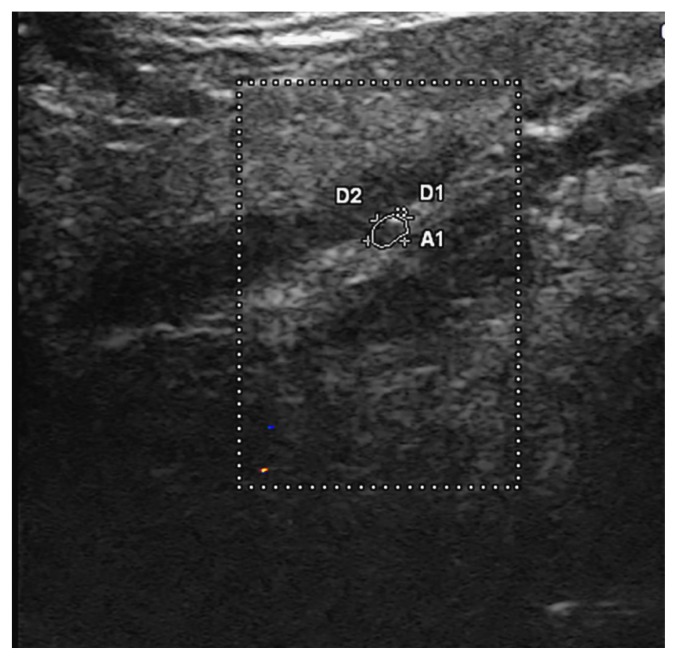
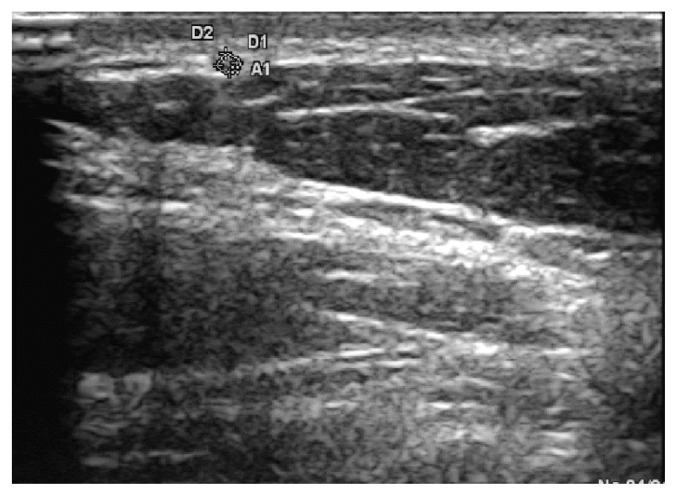
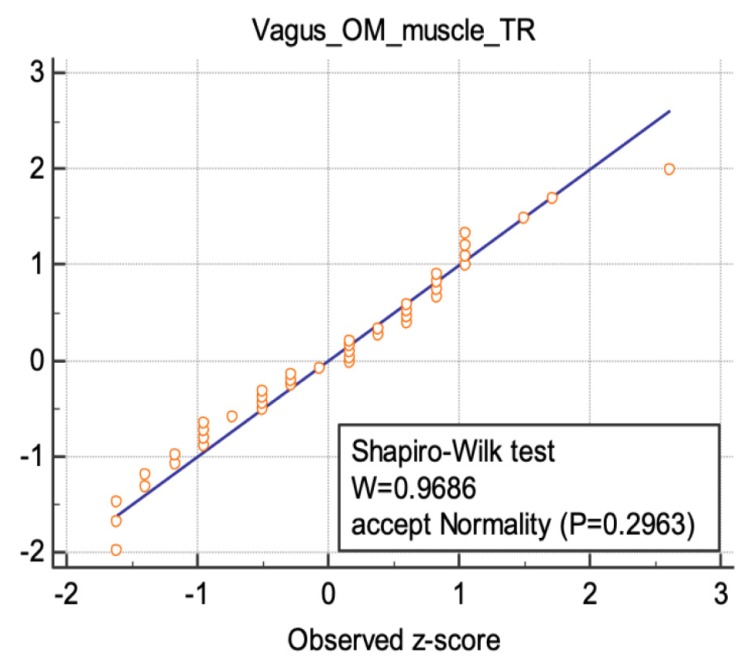
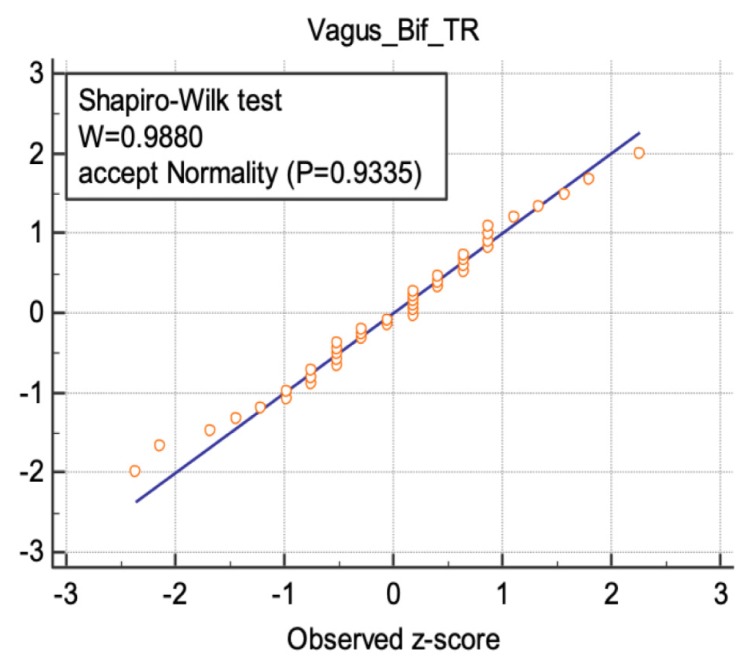
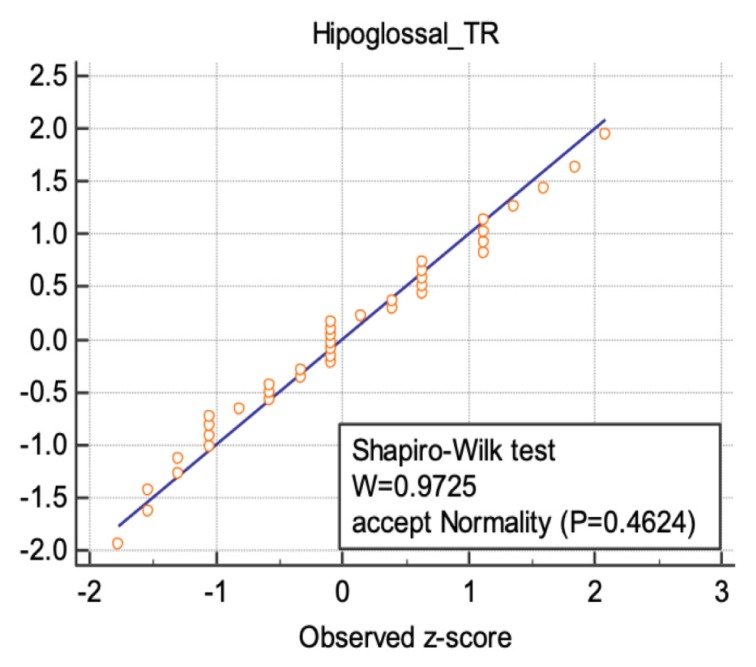
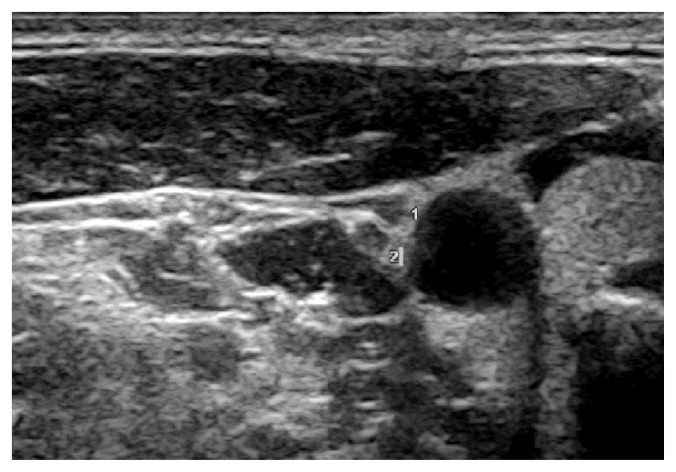
A prospective study was carried out on 21 healthy volunteers (12 women and 9 men), recording their demographic characteristics. A 13 MHz transducer was used on a Hitachi EUB-8500 machine. The vagus nerve was measured at the bifurcation of common carotid artery (CCA) and at the intersection of the internal jugular vein with omohyoid muscle. The hypoglossal nerve was identified as it crosses the posterolateral border of the mylohyoid muscle in the submandibular space. The auricular nerve was identified on the superficial surface of the sternocleidomastoid muscle at 1 cm from its posterior margin. The mean CSA on axial scans, nerve width and thickness were determined. The side-to-side and gender differences of the estimated reference values and their correlations with the weight, height, and body mass index (BMI) were evaluated.
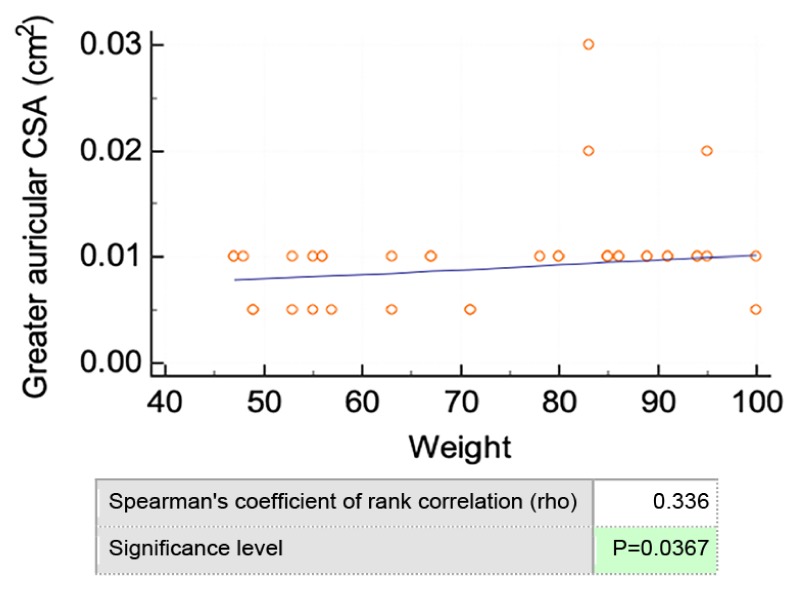
The mean ultrasound-estimated CSA was measured for the vagus nerve at CCA bifurcation (2.14 ± 0.79 on the left 2.86 ± 1.27 on the right), vagus nerve at the level of omohyoid muscle (2.10 ± 0.06 on the left and 2.43 ± 0.08 on the right), hypoglossal nerve (1.71 ± 0.08 on the left, 1.24 ± 0.06 on the right) and greater auricular nerve (0.90 ± 0.53 on the left and 0.79 ± 0.71 on the right). The vagus nerve was significantly larger on the right side compared to the left side. Larger hypoglossal nerve was observed in men compared to women. Significant correlations were observed between weight and CSA of the greater auricular nerve.
Direct visualization of the vagus, greater auricular nerve and hypoglossal nerves is feasible. Reference values for the size of the studied nerves at specific anatomic landmarks were established. Side, gender and body weight differences of the nerves CSA were noted.
超声检查中关于神经参考值的信息,尤其是颈部神经的参考值信息有限。本研究的目的是证明直接可视化迷走神经、舌下神经和耳大神经的可行性,在健康志愿者身上测试该方法,并估计两条垂直直径和横截面积(CSA)的参考值。
对21名健康志愿者(12名女性和9名男性)进行了一项前瞻性研究,记录他们的人口统计学特征。在日立EUB - 8500机器上使用13 MHz探头。在颈总动脉(CCA)分叉处和颈内静脉与肩胛舌骨肌的交叉处测量迷走神经。舌下神经在颌下间隙穿过下颌舌骨肌后外侧缘时被识别。在胸锁乳突肌后缘1 cm处的表面识别耳大神经。确定轴向扫描上的平均CSA、神经宽度和厚度。评估估计参考值的左右差异和性别差异,以及它们与体重、身高和体重指数(BMI)的相关性。
在CCA分叉处,迷走神经的平均超声估计CSA为(左侧2.14±0.79,右侧2.86±1.27);在肩胛舌骨肌水平,迷走神经的平均超声估计CSA为(左侧2.10±0.06,右侧2.43±0.08);舌下神经为(左侧1.71±0.08,右侧1.24±0.06);耳大神经为(左侧0.90±0.53,右侧0.79±0.71)。右侧迷走神经明显大于左侧。男性的舌下神经比女性的大。耳大神经的体重与CSA之间存在显著相关性。
直接可视化迷走神经、耳大神经和舌下神经是可行的。建立了特定解剖标志处研究神经大小的参考值。记录了神经CSA的左右、性别和体重差异。