Din Shah Naseer Ue, Ali Md Niamat, Ganai Bashir A, Mudassar Syed, Khan Mosin Saleem, Kour Jasbir, Waza Ajaz Ahmad, Rasool Malik Tariq, Lone Aabid Maqbool
Cytogenetic and Molecular Biology Research Laboratory, Centre of Research for Development, University of Kashmir, Srinagar, 190006, J&K, India.
Biochemistry Research Laboratory, Centre of Research for Development, University of Kashmir, Srinagar, 190006, J&K, India.
Heliyon. 2020 Feb 26;6(2):e03488. doi: 10.1016/j.heliyon.2020.e03488. eCollection 2020 Feb.
Non-small cell lung carcinoma (NSCLC) incidence and progression is increasing because of genetic and epigenetic changes. The mutations in the Kirsten rat sarcoma () are the most frequently oncogene aberrations in lung carcinoma patients. A candidate tumor suppressor gene (TSG) Ras Association Domain Family 1 Isoform A (), is silenced by promoter hypermethylation in several human malignancies including non-small cell lung carcinoma (NSCLC). We hypothesized that methylation and mutations may play an important role in NSCLC.
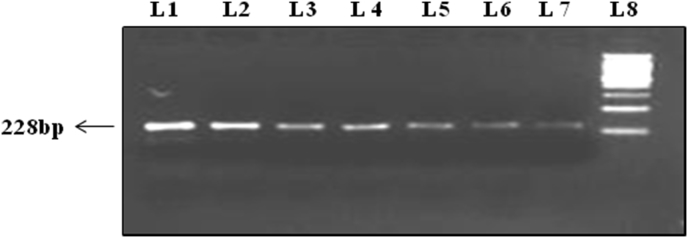
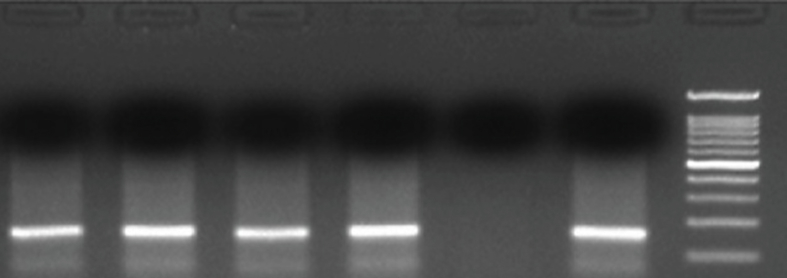
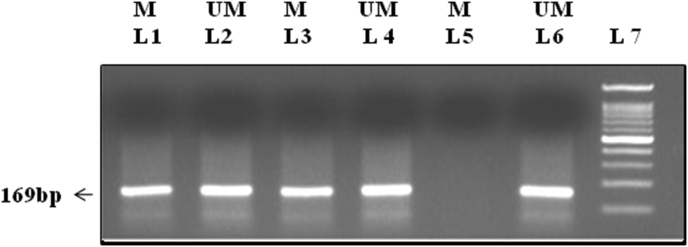
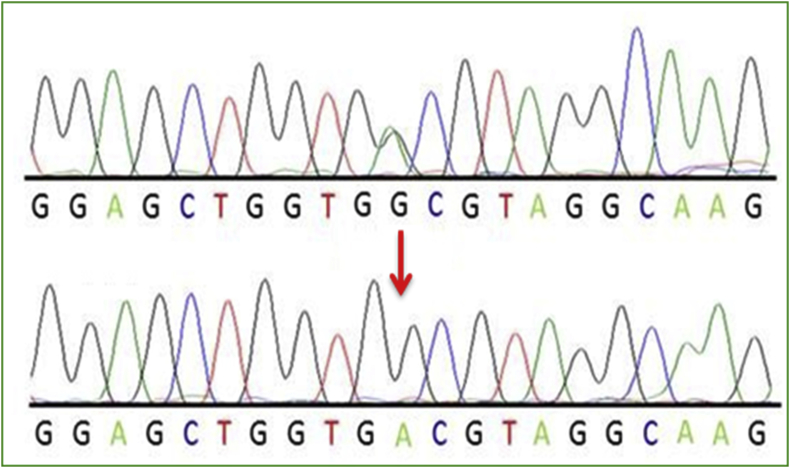
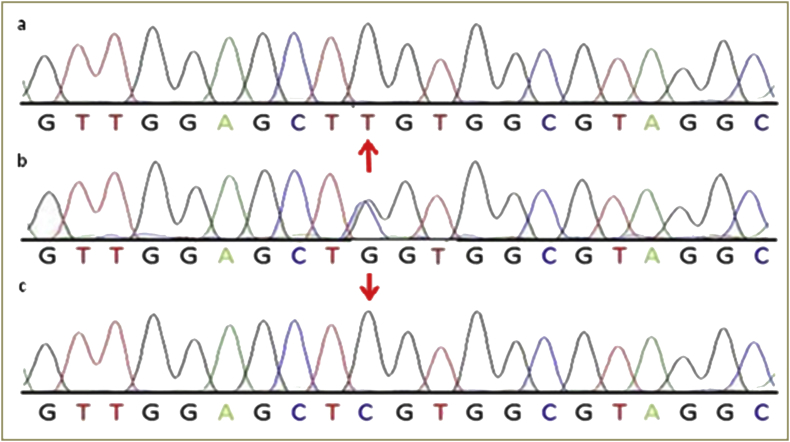
Non-small cell lung carcinoma patients (n = 100) and equal number of healthy controls were assessed for activating (exon 2) mutations using allele-specific oligonucleotide polymerase chain reaction (ASO-PCR) and promoter hypermethylation of using methylation specific PCR.
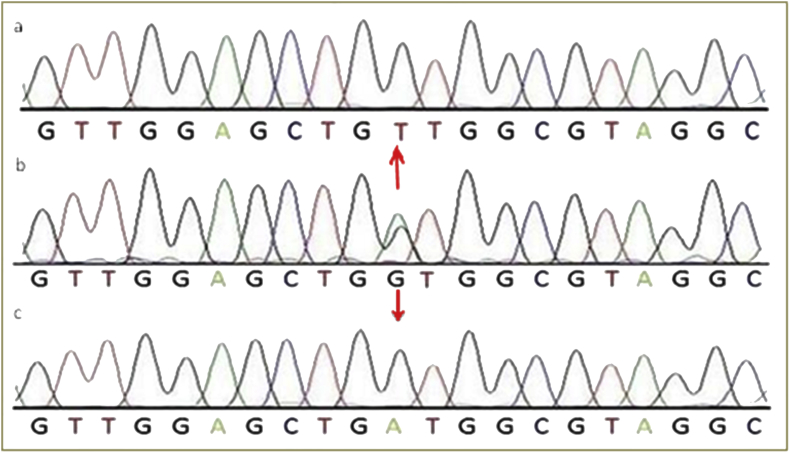
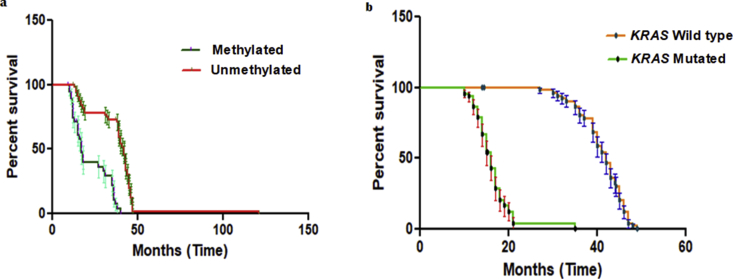
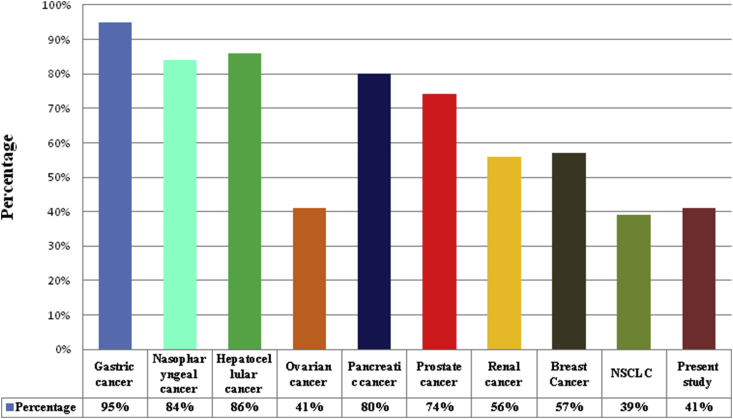
The frequency of mutations in Kirsten rat sarcoma () were found in 31% of NSCLC patients in the Kashmiri population and occur most commonly, but not exclusively, in adenocarcinoma histology and life-long smokers. The NSCLC patients in advanced stage reported the higher frequency of mutation in (exon 2). A significant higher frequency of this mutation was reported in patients with NSCLC (29.16%) who are positive for metastasis ( < 0.03). The frequencies of promoter hypermethylation at Ras Association Domain Family 1 Isoform A () were 41% in cases and 3% in control samples. The frequency of mutation and promoter methylation were significantly different between adenocarcinomas (ADC) and squamous cell carcinomas (SCC) patients with NSCLC ( < 0.03). In addition, we reported that NSCLC patients having promoter methylation was significantly associated with smoking ( = 0.01). It was identified that NSCLC patients with promoter region hypermethylation had poorer survival and faster disease progression compared with those without hypermethylation of promoter region ( = 0.0001). The Median survivals among with cases containing promoter region hypermethylation of were 17.20 and 42.13 months for patients without promoter region hypermethylation of and the patients with mutation with or without hypermethylation of the promoter region of a tumor suppressor gene had poorer survival compared with those patients with wild type gene, with or without hypermethylation of promoter region. These differences were statistically significant based on Log-rank (Mantel-cox) test ( = 0.0001). The median survivals among patients with mutation in protooncogene were 16 months and 42 months for NSCLC patients with wild type gene.
The aberrant gene promoter methylation with the subsequent mutation in gene (exon 2) plays a significant role in the pathogenesis and disease progression of non-small cell lung carcinoma (NSCLC).
由于基因和表观遗传变化,非小细胞肺癌(NSCLC)的发病率和进展呈上升趋势。 Kirsten 大鼠肉瘤()突变是肺癌患者中最常见的致癌基因畸变。候选肿瘤抑制基因(TSG)Ras 关联结构域家族 1 亚型 A()在包括非小细胞肺癌(NSCLC)在内的几种人类恶性肿瘤中因启动子高甲基化而沉默。我们假设甲基化和突变可能在 NSCLC 中起重要作用。
使用等位基因特异性寡核苷酸聚合酶链反应(ASO-PCR)评估 100 例非小细胞肺癌患者和同等数量的健康对照的激活(外显子 2)突变,并使用甲基化特异性 PCR 评估的启动子高甲基化。
在克什米尔人群的 31%的 NSCLC 患者中发现了 Kirsten 大鼠肉瘤()突变,最常见于腺癌组织学和终身吸烟者,但并非仅见于这些情况。晚期 NSCLC 患者报告的(外显子 2)突变频率更高。在转移呈阳性的 NSCLC 患者(<0.03)中,该突变的频率明显更高(29.16%)。Ras 关联结构域家族 1 亚型 A()启动子高甲基化的频率在病例中为 41%,在对照样本中为 3%。NSCLC 腺癌(ADC)和鳞状细胞癌(SCC)患者之间的突变频率和启动子甲基化频率有显著差异(<0.03)。此外,我们报告 NSCLC 患者启动子甲基化与吸烟显著相关(=0.01)。已确定启动子区域高甲基化的 NSCLC 患者与未发生启动子区域高甲基化的患者相比,生存率更低,疾病进展更快(=0.0001)。启动子区域高甲基化的病例中,未发生启动子区域高甲基化的患者的中位生存期为 17.20 个月,发生启动子区域高甲基化或未发生启动子区域高甲基化的突变患者的中位生存期为 42.13 个月。与野生型基因的患者相比,无论启动子区域是否高甲基化,肿瘤抑制基因启动子区域高甲基化或未高甲基化的突变患者的生存率更低。基于对数秩(Mantel-cox)检验,这些差异具有统计学意义(=0.0001)。原癌基因突变的 NSCLC 患者中,野生型基因的患者的中位生存期为 16 个月和 42 个月。
异常的基因启动子甲基化以及随后的基因(外显子 2)突变在非小细胞肺癌(NSCLC)的发病机制和疾病进展中起重要作用。