Bakhru Rita N, Davidson James F, Bookstaver Rebeca E, Kenes Michael T, Peters Stephen P, Welborn Kristin G, Creech Oksana R, Morris Peter E, Files D Clark
Department of Internal Medicine, Section on Pulmonary, Critical Care, Allergy, and Immunological Diseases, Wake Forest School of Medicine, Winston-Salem, NC.
Critical Illness Injury and Recovery Research Center, Wake Forest University, Winston-Salem, NC.
Crit Care Explor. 2019 Aug 9;1(8):e0034. doi: 10.1097/CCE.0000000000000034. eCollection 2019 Aug.
Post-ICU clinics may facilitate the care of survivors of critical illness, but there is a paucity of data describing post-ICU clinic implementation. We sought to describe implementation of our ICU recovery clinic, including an assessment of barriers and facilitators to clinic attendance.
Adults admitted to the medical ICU of a large tertiary care academic hospital with shock and/or respiratory failure requiring mechanical ventilation were screened for participation in a newly formed ICU recovery clinic. Participant selection and attendance rates were tracked. Reasons for nonattendance were assessed by phone call in a subset of patients.
A newly formed ICU recovery clinic of a large tertiary care academic hospital.
All patients admitted to the medical ICU were screened.
ICU recovery clinic appointments were scheduled for all eligible patients. A subset of nonattenders were called to assess reasons for nonattendance.
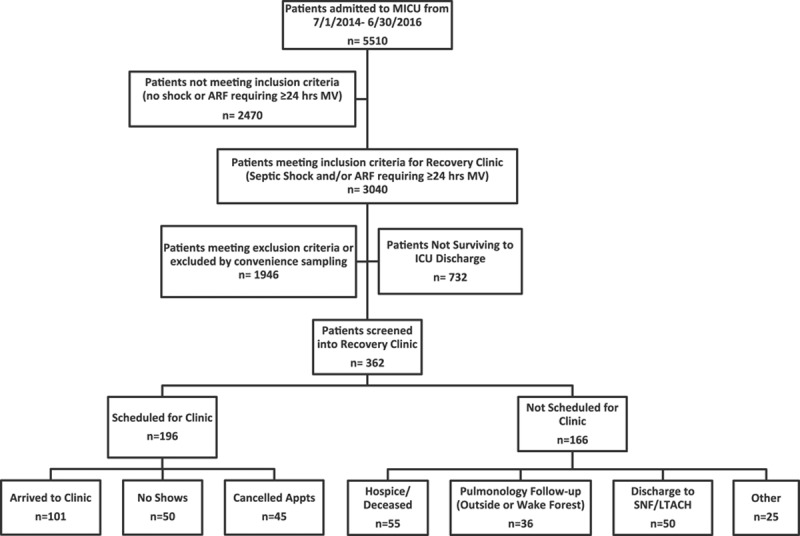
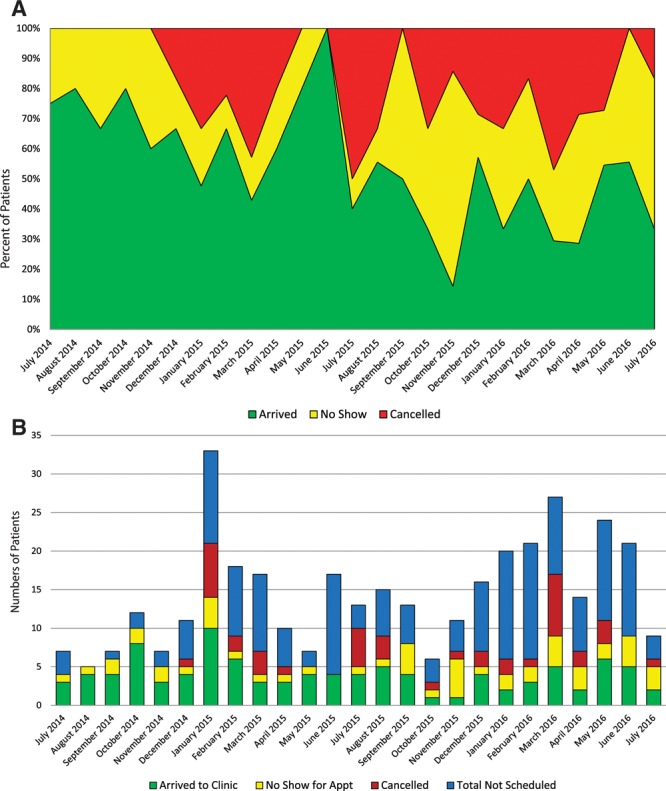
Over 2 years, we admitted 5,510 patients to our medical ICU. Three hundred sixty-two were screened into the recovery clinic. One-hundred sixty-six were not scheduled for clinic; major reasons included discharge to hospice/death in the hospital ( = 55) and discharge to a facility ( = 50). One-hundred ninety-six patients were scheduled for a visit and of those, 101 (52%) arrived to clinic. Reasons for nonattendance in a surveyed subset of nonattenders included patient's lack of awareness of the appointment (50%, = 9/18), financial concerns (17%, = 3/18), and transportation difficulty (17%, = 3/18).
ICU recovery clinics may address the needs of survivors of critical illness. Barriers to clinic attendance include high mortality rates, high rates of clinic appointment cancelations and nonattendance, and discharge to locations such as skilled nursing facilities or long-term acute care hospitals. Improved communication to patients about the role of the clinic may facilitate attendance and minimize canceled appointments.
重症监护病房后门诊可能有助于危重病幸存者的护理,但描述重症监护病房后门诊实施情况的数据很少。我们试图描述我们的重症监护病房康复门诊的实施情况,包括评估门诊就诊的障碍和促进因素。
对入住一家大型三级医疗学术医院内科重症监护病房、因休克和/或呼吸衰竭需要机械通气的成年人进行筛查,以确定其是否参与新成立的重症监护病房康复门诊。跟踪参与者的选择和就诊率。通过电话对一部分患者评估未就诊的原因。
一家大型三级医疗学术医院新成立的重症监护病房康复门诊。
对入住内科重症监护病房的所有患者进行筛查。
为所有符合条件的患者安排重症监护病房康复门诊预约。对一部分未就诊者进行电话随访以评估未就诊原因。
在两年多的时间里,我们内科重症监护病房收治了5510名患者。362名患者被筛查进入康复门诊。166名患者未安排门诊就诊;主要原因包括转至临终关怀机构/在医院死亡(n = 55)和转至其他机构(n = 50)。196名患者被安排就诊,其中101名(52%)前来门诊。在接受调查的未就诊者子集中,未就诊的原因包括患者对预约不知情(50%,n = 9/18)、经济担忧(17%,n = 3/18)和交通困难(17%,n = 3/18)。
重症监护病房康复门诊可能满足危重病幸存者的需求。门诊就诊的障碍包括高死亡率、门诊预约取消率和未就诊率高,以及转至诸如熟练护理机构或长期急性护理医院等场所。改善与患者关于门诊作用的沟通可能有助于提高就诊率并减少预约取消。