Miguel-Esponda Georgina, Bohm-Levine Nathaniel, Rodríguez-Cuevas Fátima Gabriela, Cohen Alex, Kakuma Ritsuko
1Centre for Global Mental Health, Department of Population Health, Faculty of Epidemiology & Population Health, London School of Hygiene & Tropical Medicine, Keppel Street, London, WC1E 7HT UK.
2University of California, San Francisco, USA.
Int J Ment Health Syst. 2020 Mar 16;14:21. doi: 10.1186/s13033-020-00346-x. eCollection 2020.
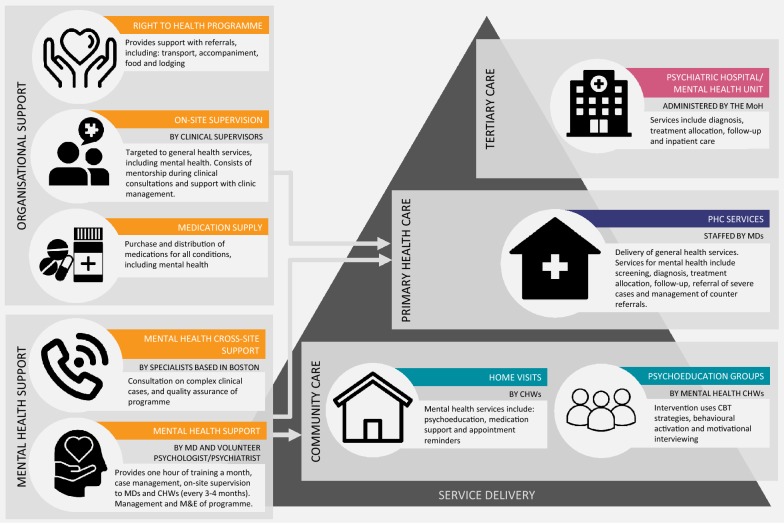
Policies and programmes in Mexico promote the integration of mental health services into primary health care (PHC), however these services remain largely unavailable in the country. Since 2014 a non-governmental organisation has delivered a mental health programme at PHC clinics in the state of Chiapas, in partnership with the local Ministry of Health (MoH). The programme provides mental health services based on the mhGAP guidelines through multiple implementation strategies, including programme financing, infrastructure strengthening, high-intensity training, and supervision. This study aimed to examine the implementation process and outcomes of this mental health programme to understand the extent to which mental health care integration has been achieved and to identify the successes and remaining challenges in order to inform the development and implementation of similar programmes.
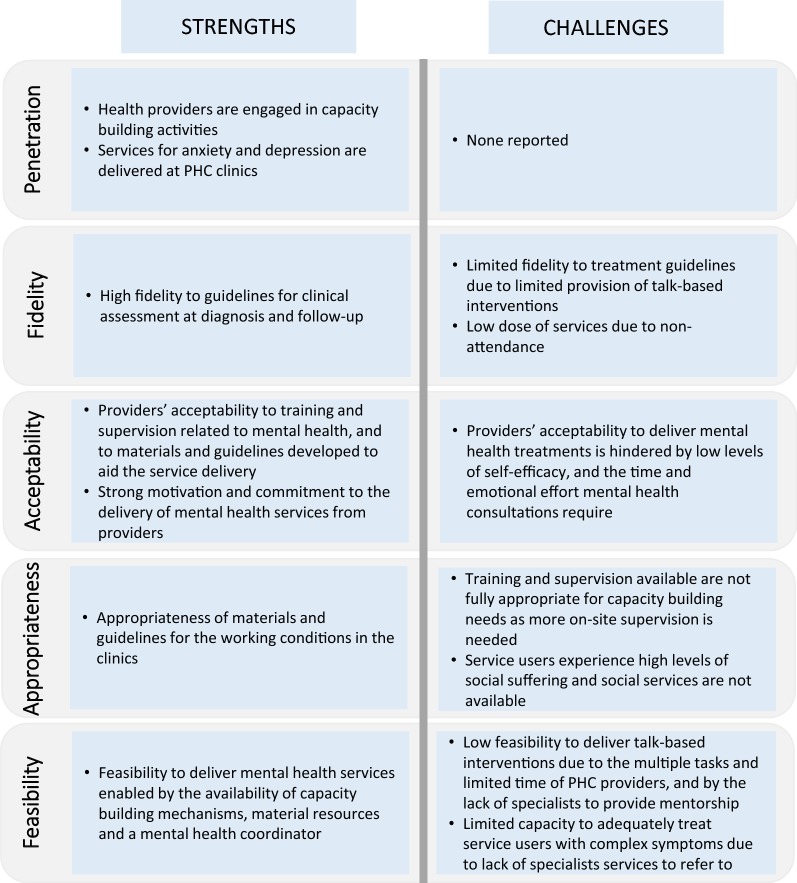
We used a mixed-methods convergent design. Quantitative data for the period between December 2016 and December 2017 were extracted from the organisation's health information system to capture process indicators, including the amount (dose) and quality (fidelity) of services delivered. We conducted two focus groups and 24 semi-structured interviews with health providers and managers to ascertain implementation outcome data: penetration, fidelity, acceptability, appropriateness and feasibility. Quantitative and qualitative data were analysed using descriptive and framework analyses, respectively.
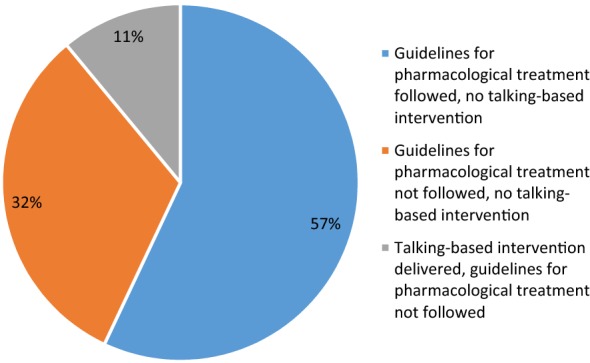
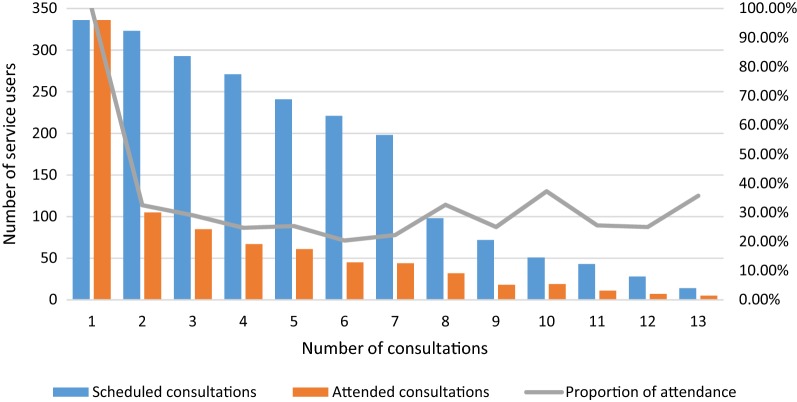
During the study period, health providers delivered mental health consultations to 486 adults diagnosed with a mood or anxiety disorder. Programme fidelity was limited given that talk-based interventions, which are required in all consultations according to programme guidelines, were only provided in 24% of consultations. Only 42% of service users attended more than 50% of scheduled mental health follow-up consultations, which also hindered fidelity. Low attendance is partially attributed to limited programme appropriateness, given that interventions to address social risk factors are not available. High levels of acceptability and feasibility enabled through strong support from the organisation were key programme strengths.
Mental health programmes at PHC can be implemented when adequate support and supervision structures are in place, and key resources are available. There is an urgent need for health systems strengthening to support efforts to provide mental health care, and to link PHC with locally-relevant social interventions.
墨西哥的政策和项目推动将精神卫生服务纳入初级卫生保健(PHC),然而该国这些服务在很大程度上仍然难以获得。自2014年以来,一个非政府组织与恰帕斯州当地卫生部(MoH)合作,在该州的初级卫生保健诊所开展了一项精神卫生项目。该项目通过多种实施策略,包括项目融资、基础设施强化、高强度培训和监督,依据mhGAP指南提供精神卫生服务。本研究旨在考察该精神卫生项目的实施过程和结果,以了解精神卫生保健整合的实现程度,并确定成功之处和尚存的挑战,为类似项目的开发和实施提供信息。
我们采用了混合方法收敛设计。从该组织的健康信息系统中提取了2016年12月至2017年12月期间的定量数据,以获取过程指标,包括提供服务的数量(剂量)和质量(保真度)。我们对卫生服务提供者和管理人员进行了两个焦点小组讨论和24次半结构化访谈,以确定实施结果数据:渗透率、保真度、可接受性、适宜性和可行性。分别使用描述性分析和框架分析对定量和定性数据进行分析。
在研究期间,卫生服务提供者为486名被诊断患有情绪或焦虑障碍的成年人提供了精神卫生咨询。鉴于根据项目指南所有咨询都需要的基于谈话的干预措施仅在24%的咨询中提供,项目保真度有限。只有42%的服务使用者参加了超过50%的预定精神卫生随访咨询,这也妨碍了保真度。就诊率低部分归因于项目适宜性有限,因为缺乏解决社会风险因素的干预措施。该组织的大力支持所带来的高度可接受性和可行性是项目的关键优势。
当有适当的支持和监督结构且有关键资源可用时,初级卫生保健中的精神卫生项目可以实施。迫切需要加强卫生系统,以支持提供精神卫生保健的努力,并将初级卫生保健与当地相关的社会干预措施联系起来。