University of Rwanda, College of Medicine and health sciences, Kigali, Rwanda.
University Hospital of Brooklyn, SUNY Downstate Medical Center, Brooklyn, NY, USA.
BMC Infect Dis. 2020 Mar 20;20(1):239. doi: 10.1186/s12879-020-04965-0.
Peritoneal tuberculosis is the most common cause of low albumin gradient ascites in developing countries, but it can be easily confused with other causes of ascites. Peritoneal tuberculosis requires early recognition of symptoms and signs in order to make a quick diagnosis for appropriate treatment. Measurement of adenosine deaminase (ADA) level > 39 in ascites fluid is an established test to diagnose peritoneal tuberculosis. Many low-income countries do not currently test for adenosine deaminase in ascites fluid, including Rwanda.
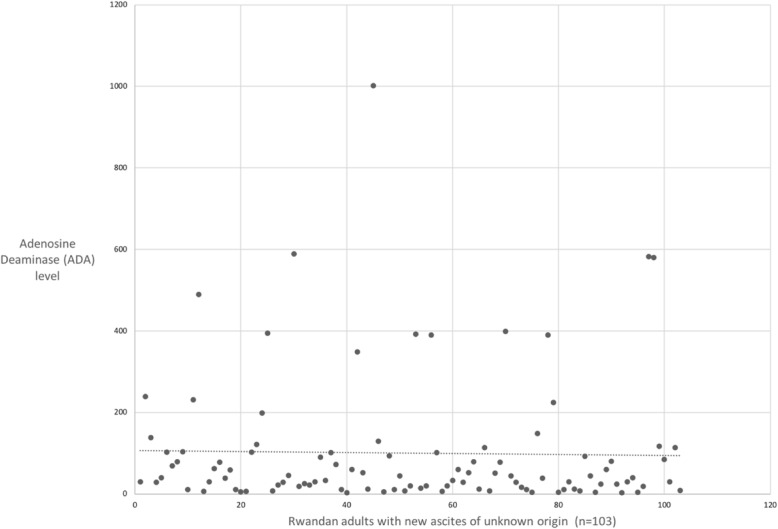
Cross-sectional, descriptive study conducted through the Internal Medicine Department of three university teaching hospitals in Rwanda. Participants were patients older than 16 years presenting to tertiary referral hospitals with ascites of unknown cause.
Of 103 ascites fluid samples collected, 52 of them (50.5%) had an elevated ADA, consistent with a presumptive diagnosis of peritoneal TB. Among those 52 subjects diagnosed with peritoneal TB, 39 out of 52 (75%) did not receive anti-TB medications. Among the 17 subjects who were treated with anti-TB medications, 4 of 17 (23.6%) did not have peritoneal TB based on ADA level. Samples with low-albumin gradient ascites were more likely to have high ADA ≥39 IU/L (p = 0.039).
Our findings suggest that 3out of 4 patients with PTB in Rwanda are not getting TB treatment and 1 in 4 patients who are taking TB medications do not need it. Even if the true number of Rwandans who are being undertreated and overtreated is less than our study suggests, these results should prompt a larger study of peritoneal tuberculosis. Adding adenosine deaminase (ADA) to the diagnostic tools available to clinicians could help achieve the goal of correctly putting every Rwandan with tuberculosis on treatment, while avoiding unnecessary tuberculosis medications in those who do not have the disease.
在发展中国家,腹膜结核是导致低白蛋白梯度腹水的最常见原因,但它很容易与其他腹水原因混淆。腹膜结核需要早期识别症状和体征,以便快速诊断并进行适当治疗。腹水腺苷脱氨酶(ADA)水平>39 是诊断腹膜结核的既定检测方法。许多低收入国家目前并未检测腹水 ADA,包括卢旺达。
在卢旺达的三家大学教学医院的内科进行横断面描述性研究。参与者为年龄大于 16 岁的腹水病因不明的患者,他们到三级转诊医院就诊。
共收集了 103 份腹水样本,其中 52 份(50.5%)ADA 升高,符合腹膜结核的初步诊断。在这 52 名被诊断为腹膜结核的患者中,39 名(75%)未接受抗结核药物治疗。在接受抗结核药物治疗的 17 名患者中,有 4 名(23.6%)根据 ADA 水平并未患有结核性腹膜炎。低白蛋白梯度腹水的样本更有可能 ADA≥39IU/L(p=0.039)。
我们的研究结果表明,卢旺达 3 名结核性腹膜炎患者未接受结核病治疗,而接受结核病药物治疗的 4 名患者中有 1 名并不需要这种治疗。即使未接受治疗和过度治疗的卢旺达患者人数少于我们的研究结果所表明的,这些结果也应促使对结核性腹膜炎进行更大规模的研究。将腺苷脱氨酶(ADA)添加到临床医生可用的诊断工具中,可以帮助实现将每一位患有结核病的卢旺达患者正确治疗的目标,同时避免在那些没有结核病的患者中使用不必要的结核病药物。